Introduction
Folate, or vitamin B9, is a naturally occurring, water-soluble vitamin predominantly found in legumes, leafy green vegetables, and some citrus fruits.1 Folic acid is a synthetic dietary supplement used to increase serum folate levels. Despite these differences, literature commonly uses folate and folic acid interchangeably; folate is an umbrella term used to describe all folate derivatives. Both substances eventually produce the same intermediate necessary for the folate cycle and, by extension, the 1-carbon cycle.2 Folate enters the cycle as tetrahydrofolate (THF), whereas folic acid undergoes reduction to dihydrofolate (DHF) before it is converted to THF. Both folate and folic acid eventually produce 5-methyltetrahydrofolate (5-MTHF), the active substance used in biological processes.2 Deficiencies in this nutrient are implicated in a cascade of fetal and maternal conditions, some of which have lethal outcomes.
Based on accepted guidelines for prenatal care, pregnant individuals should have a daily regimen of prenatal folic acid supplementation.3 Adherence to this supplementation regimen ensures proper serum folate levels across populations of pregnant individuals, which is proven to decrease the incidence of neural tube defects (NTDs) and is implicated in the prevention of a variety of other conditions, including ophthalmic issues, food allergies, and deficiencies in neurodevelopment.3–6 In addition to appropriate fetal development, folic acid supplementation supports maternal health during pregnancy. The breadth of evidence indicates periconceptional folic acid intake is a critical component of the prenatal standard of care.2 This article provides a review of suspected folic acid mechanisms and outlines existing guidelines and population-based strategies to improve maternal folate levels.
Structure, Interactions, and Generalized Roles of Folic Acid
Structure of Folate
Within the body, folate exists in its active form THF. THF is converted to 5-MTHF, the predominant form of folate circulating in the blood. THF is also used as a substrate for downstream effects, including the management of homocysteine levels. Unlike folate, folic acid is not immediately biologically available post consumption and requires metabolism to THF before use in metabolic processes.7
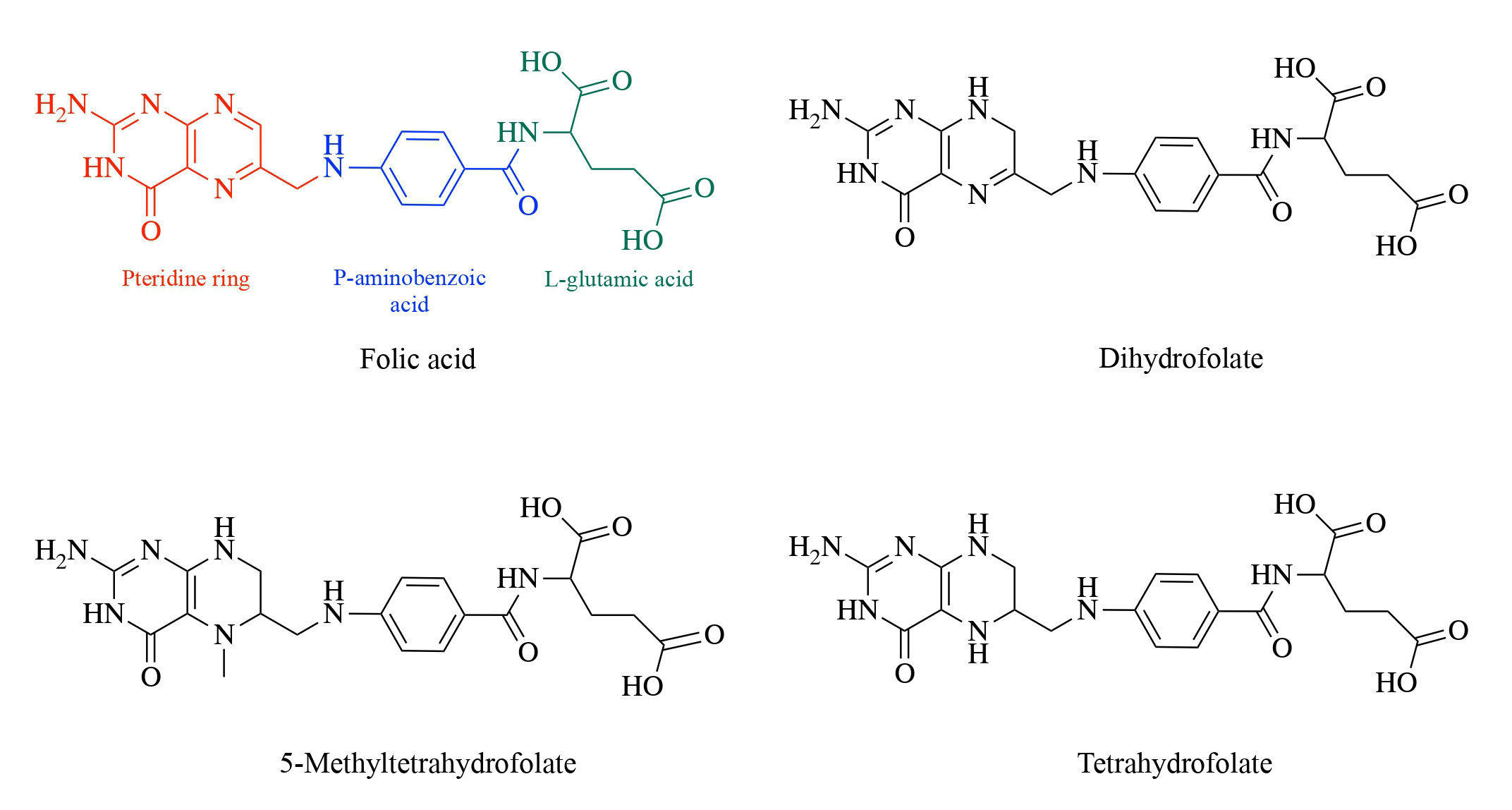
THF is a polyglutamate readily accessible to metabolic functions without extensive alteration. In comparison, folic acid enters as a monoglutamate that requires reduction by dihydrofolate reductase before participating in various functions. The structure of folic acid takes on a pteridine that is linked to a para-aminobenzoic acid and L-glutamic acid (Figure 1). Given its structure, many folic acid conjugates differ in the number of glutamic acid sequences. Furthermore, the reducibility of the pteridine ring allows the conversion of folic acid into derivative molecules, including DHF or THF.8 Both derivatives function separately but play essential roles in oxidation-reduction reactions and enzymatic interactions.

Folate Cycle
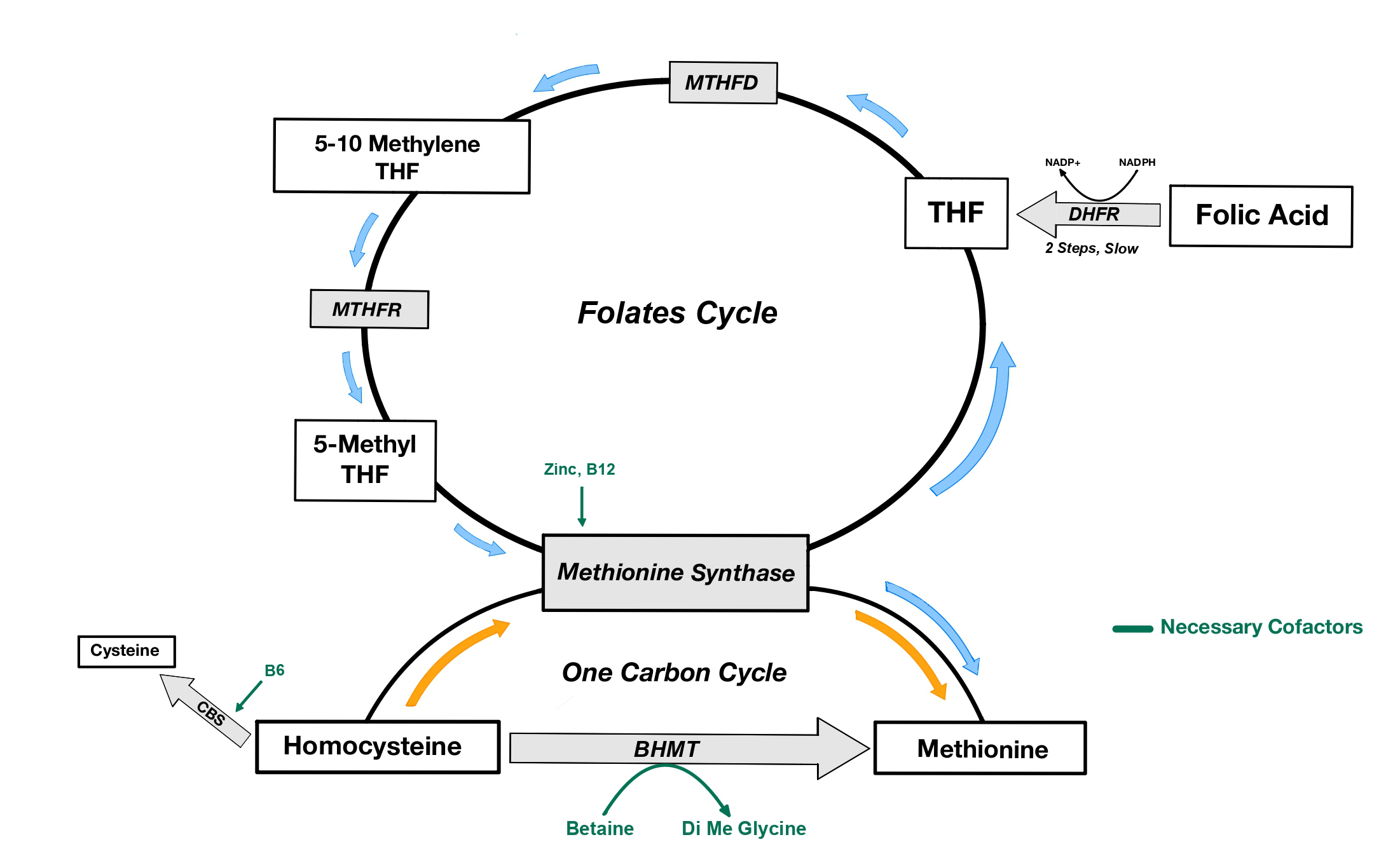
The folate cycle facilitates biological processes such as the synthesis of nucleotides, amino acids, and mitochondrial proteins. In addition, folate concentrations alter the body’s ability to epigenetically alter DNA expression via methylation processes using the methyl group donors from the 1-carbon cycle. The folate cycle provides the 1-carbon cycle with the methyl group required for the conversion of homocysteine to methionine (Figure 2). Thus, without an adequate supply of folate for the folate cycle, the 1-carbon cycle lacks the necessary substrates to promote DNA methylation.2

Supplemental folic acid must be converted to 5-MTHF to facilitate metabolic processes. In a 2-step process, folic acid is reduced to THF by the catalyzing enzyme dihydrofolate reductase with nicotinamide adenine dinucleotide phosphate (NADP) as a cofactor. THF is then converted to 5,10-methylenetetrahydrofolate (5,10-MTHF), some of which exits the folate cycle, destined to support the synthesis of nucleic acids for neurodevelopment, while the rest continues in the folate cycle to be converted to the biologically active form of folate, 5-MTHF, by methylenetetrahydrofolate reductase (MTHFR).2
1-Carbon Cycle
The 1-carbon cycle uses 5-MTHF as a substrate in converting homocysteine to methionine. Methionine synthase, a catalytic enzyme, removes a methyl group from 5-MTHF. This reaction reforms THF and exposes the newly isolated methyl group to homocysteine. The homocysteine molecule accepts the methyl group forming methionine, while the THF is recycled into the folate cycle (Figure 2). Shortages of zinc or vitamin B12, necessary cofactors of the methionine synthase reaction, result in THF and methionine deficiencies.2 Homocysteine levels are moderated by the cystathionine beta-synthase pathway and betaine homocysteine methyltransferase (BHMT). The cystathionine beta-synthase pathway converts homocysteine into cysteine, with vitamin B6 as a necessary cofactor.2 Notably, the enzymes BHMT and methionine synthase convert homocysteine into methionine using different cofactors (5-MTHF and betaine, respectively).9 While both pathways ultimately result in methionine synthesis, the BHMT pathway produces the byproduct dimethylglycine.2 Increased flux through this pathway is associated with a heightened risk of gestational diabetes and heart disease.10,11 High bioavailability of 5-MTHF facilitates the activity of methionine synthase in the conversion of homocysteine into methionine and, therefore, decreases flux through the BHMT pathway, ameliorating the risks associated with overactive BHMT.9 Higher levels of methionine increase DNA methylation and reduce oxidative stress, ensuring appropriate fetal progression during this developmental period of rapid growth.9
Interactions and Roles in Cellular Function
THF acts as a 1-carbon donor for purine and pyrimidine synthesis; its flexible structure allows for involvement in the assembly of DNA and RNA.12 Given its donor ability, folate supports cell growth, cell division, and the maintenance of new cells. Furthermore, it interacts with various cell types within the body to contribute to detoxification, promotion of energy resources, regulation of genes, and control of moods and immune responses, including inflammation.7
When consumed, folic acid transitions through several intermediates (THF and 5,10-MTHF) before converting into 5-MTHF.7 Throughout this reaction, intermediates are removed from the cycle for use in DNA/RNA synthesis or the conversion of homocysteine to cysteine in the cell. 5-MTHF is recognized by 3 receptors (FRα, FRβ, and FRγ), which are rich in cysteine glycoproteins and mediate endocytic uptake.12 Folate receptors are abundant in embryonic tissues, but their expression in healthy adult cells is minimal. These folate receptors retain responsibility for folate reabsorption in adult kidney cells and are highly concentrated within tissues responsible for embryonic development in pregnant individuals. FRα, also known as folate receptor 1, is the only receptor expressed in the preimplantation embryo, and its importance to healthy fetal development was illustrated when folate receptor 1 knockout mice exhibited deficits in cellular development, tissue development, and neural crest cell migration.13 The increased incidence of developmental disorders associated with dysfunctional FRα activity further indicates that maternal folate receptor expression plays a critical role during pregnancy and fetal development.14 Folate’s broad scope of interactions makes it a key player in multiple different facets of everyday life and health.
Folic Acid Intake
Given the direct involvement of folate in epigenetic expression, the consumption of supplemental folic acid is strongly encouraged for all women of reproductive age because it ensures adequate levels are maintained during early pregnancy. Inadequate folic acid consumption can cause deficiencies in serum folate levels; many other conditions, including decreased nutritional absorption and improper folic acid metabolism, are also potential causes for folate deficiencies.1 Regardless of the etiology, individuals with folate deficiencies require more aggressive supplementation to restore normal serum folate levels.
Folate is often stored in the liver. Thus, liver damage may disrupt the release and absorption of the molecule.1 In addition, genetic variation may exist in several genes affecting the function and metabolism of folic acid.7 A well-researched genetic polymorphism results in impaired MTHFR activity and decreased synthesis of 5-MTHF from food folates and folic acid.7,15
Measuring Folate Levels
There are a variety of options available to measure folate levels. A microbiological assay is the standard test, but protein-binding assays and mass spectrometry are also available.1 Folate concentrations can be obtained from serum/plasma levels and red blood cell levels, both indicative of varying aspects of folate concentration. Serum/plasma folate shows recent folate intake, whereas red blood cell folate is more reflective of long-term consumption. Because red blood cells require hemolysis to release the polyglutamate folate necessary for measurement, red blood cell folate levels are more challenging to collect.16
These measurements provide crucial information on circulating folic acid and aid in clinician recommendations and prescribing practices. Careful consideration must be taken when supplementing folic acid at high levels because introducing more than 200 µg of folic acid to the body results in the appearance of circulating unmetabolized folic acid (UMFA).2 Prolonged circulation of UMFA at the time of delivery could lead to adverse effects for the child that could promote possible toxic conditions.17 Integrating accurate measurement tactics with dosage advisories is critical in addressing folate deficiency concerns by collecting data to assist patient treatment and diagnosis of related conditions, including those outlined below.
Associated and Related Conditions
Deficiency in Mothers
Folate deficiencies are responsible for a variety of issues in both mothers and infants. In pregnant individuals, deficiencies in folate are responsible for the onset of macrocytosis enlargement of red blood cells, which can lead to megaloblastic anemia or pancytopenia.18 Pregnancy outcomes for individuals have been studied in the context of folate deficiencies.19 A study examining 227 pregnant individuals in Korea identified a positive correlation between homocysteine levels and the incidence of preeclampsia.19 Therefore, normal folate levels may be protective against the occurrence of preeclampsia in low homocysteine conditions. Folate deficiency can also lead to other complications such as preterm birth (birth at less than 37 weeks’ gestation) and small for gestational age (infants and fetuses at <10th percentile in weight at their respective gestational age).20 These adverse pregnancy outcomes underline the importance of maternal folic acid supplementation not only for the health of the infant, but also for the pregnant individual.
Deficiencies in Infants
Neurobehavioral Outcomes
Deficiencies in maternal folic acid have a pronounced effect on fetal development. Mice models have demonstrated a correlation between periconceptional folic acid deficiency and poor neurodevelopment, decreasing overall brain mass and increasing negative behaviors.21 Following this, large cohort studies in the Rhea population of Crete, Greece, examined maternal folic acid supplementation and the child’s neurodevelopment.6 Using the third edition of the Bayley Scales of Infant and Toddler Development to assess neural and psychomotor development, receptive communication and expressive communication scores improved by 5 and 3.5 points, respectively, in children of mothers taking at least 5 mg of folic acid compared with those taking no folic acid.6 These statistically significant improvements reflect elevated communication skills compared with control, a direct correlate of neurobehavioral development. Additionally, a large cohort-style study from Norway showed that children whose mothers used periconceptional folic acid supplementation, either alone or in combination with another supplement, were less likely to develop a severe language delay compared with children of mothers who did not use periconceptional supplementation.22 These findings across different demographic groups suggest that folate plays a crucial role in neurobehavioral maturation in infants.
Food Allergies
Total folate levels have been associated with the incidence of food allergies. A group of nearly 1400 US children, roughly 40% of whom had some food intolerance or allergy, were studied for maternal folate levels at birth; folate levels were 14% lower in mothers of children with food allergies and intolerances. Additionally, maternal folate concentrations in the third quartile (30.4-44.8 nmol/L) were associated with a lower risk of infant food allergies compared with those in the first quartile (6.64-19.7 nmol/L).3 This research supports moderate folate levels as protective against food allergies. Conversely, abnormally high folate levels resulted in increased levels of UMFA, which may increase the risk of food allergies.3 While research has shown a correlation between food allergies and maternal folic acid supplementation, the biochemical basis is unknown, and further research is required to uncover an underlying mechanism.
Ophthalmic Development
There is a close relationship between the development of the nervous and ophthalmic systems due to the shared gene pool in the development of the optic pits and neural tube, which form in the embryo around week 4.5 Studies in mouse models showed that a diet deficient in folic acid for 2 weeks following gestation and 6 weeks before pregnancy showed an increase in the incidence of microphthalmia and thickening of the cornea compared with the control.5 This was associated with overexpression of type IV collagen and laminin-1, 2 proteins involved in the formation of the basal lamina of the eye,5 suggesting that folate’s DNA methylation capabilities play a key role in ophthalmic and neurologic development and are likely involved in other systems as well. Research is limited in this space, and further studies should expand on the current literature’s work examining the effects of high folic acid supplementation on ophthalmic development.
Clinical Picture of NTDs
NTDs are the most common congenital malformation associated with folate deficiency. NTDs are caused by a failure of neural tube fusion at week 4 of embryogenesis.23 Among NTDs, the 2 most common are anencephaly, failure of the cranial neural tube to fuse, and myelomeningocele, failure of the neural tube in the spinal region to fuse; these 2 are part of a category of NTDs known as open NTDs due to the exposure of the neural tube to the dorsal surface.23 Anencephaly and myelomeningocele are the most lethal NTDs, with mortality rates close to 100% for untreated cases.23 Closed NTDs, with no exposure to the body surface, include encephalocele, spinal dysraphism (better known as spina bifida occulta), meningocele, iniencephaly, and lipomeningocele.23
Suspected Genetic Mechanism of NTDs
Although the exact mechanism of the formation of NTDs remains unknown, a recent study tied the enzyme DOT1-like histone lysine methyltransferase (DOT1L) to methylation on H3 lysine position H3K79me2.24 Differential methylation, at this location and others, is involved in gene expression during the stages of embryonic development. H3k79me2 has been implicated in development because it is upregulated in the presence of genes found later in maturation.25 In analyzed NTD samples, DOT1L was downregulated, and low levels of H3K79me2 were found. Furthermore, a decrease in H3K79me2 results in decreased expression of both Shh and Sufu in mice. Shh and Sufu expression was also decreased in the presence of a folate antagonist, where DOT1L concentrations and H3K79me2 expression were reduced. Analysis of tissue samples found a correlation between the downregulation of Shh and Sufu and NTDs. Further analysis of the samples showed a positive correlation between the epigenetic expression of Shh and Sufu and the protein concentrations of DOT1L.24 These findings point to DOT1L-controlled H3K79me2 levels directly influencing Shh and Sufu expression and a potential mechanism for NTDs. By extension, the effects of folate on DOT1L expression likely have a direct impact on the incidence and prevention of NTDs through this mechanism.
Complications of Excess Folic Acid
Dihydrofolate reductase, the enzyme that converts folic acid to THF, has a low catalytic rate in humans compared with other species.26 This comparatively low rate of conversion, coupled with overconsumption of folic acid, can result in a build-up in UMFA. UMFA can adversely affect the body because it may compete with naturally metabolized 5-MTHF for the folate transporters SLC19A1 and folate receptor 1. Thus, increased UMFA concentrations function to lower available folate and inhibit the integrated folate cycle and 1 carbon metabolic cycle.2 High levels of UMFA in children have been associated with a higher risk of autism and food allergies.3
Genetic variation alters the metabolic rate of folic acid in certain individuals. MTHFR, the enzyme converting THF to 5-MTHF, is subject to single-nucleotide polymorphisms. These variants may result in lower expression of MTHFR and lower production of 5-MTHF. The clinical implications of insufficient 5-MTHF production are lower serum folate levels that place these individuals and their infants at risk for any of the aforementioned complications.15 This 5-MTHF deficiency arrests the 1-carbon cycle, leading to a buildup of homocysteine and a lack of recycled THF. Notably, high levels of homocysteine due to this genetic variation are predominantly found in men due to the protective effect of elevated estrogen levels in women, leading to an upregulation of the cystathionine beta-synthase pathway and BHMT.9 Researchers hypothesized that this estrogen-dependent mechanism reduces the risk of hyperhomocysteinemia and protects the developing embryo from oxidative stress. Hyperhomocysteinemia is associated with mitochondrial dysfunction27 and increased cardiovascular, cerebrovascular, and thromboembolic pathologies.28
Both indirect interference with the 1-carbon cycle via lower flux through the folate pathway and direct interference with methionine synthase inhibit the ability to methylate DNA. The application of methyl tags on DNA is necessary to fortify against oxidative stress in the body.2 This interference is the likely mechanism for many folate deficiency–associated conditions. Both low folate levels and excess UMFA levels have been found to alter DNA methylation, resulting in significant consequences on fetal outcomes. Appropriate maternal folic acid supplementation, within the proper range, aids embryonic development and protects against unfavorable outcomes later in life.2
Implications
Recommendations and Alternatives for Folate Supplementation
Folate levels in blood decrease significantly during normal pregnancy; the physiologic basis for this decline has been well documented in obstetric medicine and is linked to the fetus’ preferential use of folic acid.3 As previously established, without proper action to correct this deficiency, low folate levels are strongly associated with multiple pathologic conditions for both mother and baby. Research dating to the 1960s established the necessity of folic acid supplementation during pregnancy, recommending a minimum daily intake of 300 µg (0.3 mg) on top of the baseline dietary folic acid.29 The most recent World Health Organization (WHO) recommendation suggests all women trying to conceive begin daily oral folic acid supplementation at 400 µg (0.4 mg) and maintain this level throughout their pregnancy.16 Furthermore, the WHO recommends that pregnant individuals who receive an NTD diagnosis for their fetus be advised to both increase their dietary folic acid intake and supplement with a high-dose folic acid vitamin (5 mg).16 The U.S. Preventive Services Task Force recommends all women who plan to become pregnant take a daily folic acid supplement (0.4-0.8 mg) as a Grade A recommendation, meaning they have identified a substantial benefit and minimal harm of folic acid supplements in this population supported by ample research.30,31 The U.S. National Institutes of Health Office of Dietary Supplements recognizes the health risks associated with excessive folate and reports a tolerable upper intake level for folic acid at 1000 µg (1 mg).32 This recommendation coincides with the existing research regarding the adverse effects of high levels of UMFA. The strength of this research base is generally accepted by the pharmaceutical industry, as evidenced by the number of folic acid supplements on the market; 98% of commercial prenatal vitamins contain folate, with 95% meeting or exceeding the 400-µg recommended level.3
In addition to the published supplementation recommendations from national health organizations, many countries have instituted folic acid fortification requirements in certain food industries. In 1998, the US Food and Drug Administration created an enrichment specification that requires folic acid’s inclusion in all cereal grain products labeled “enriched.31” The U.S. Centers for Disease Control and Prevention maintains that mandatory fortification is the best public health strategy to eliminate NTDs because of its broad influence on the entire population; specifically, this strategy enhances folate levels during the first weeks of pregnancy before a woman takes a pregnancy test and begins prenatal care.31,33 The National Health and Nutrition Examination Survey found a significant linear increase in population serum and red blood cell folate levels post fortification, followed by a slight decrease during the 12-year study period.34 Despite the subsequent decline, this initiative is ultimately considered successful as folic acid in foods prevents about 1300 neural tube defects in the U.S. annually.31 The benefits of folic acid fortification are believed to be independent of demographic subgroups, which further supports its importance and may help to minimize maternal and child health disparities.34 Voluntary fortification of traditionally Hispanic foods, such as corn masa flour, recently began in the US in an attempt to reduce the folic acid disparity among Hispanic mothers. Data on the efficacy of this initiative does not yet exist; however, it is estimated to prevent an additional 40 infants from being born with NTDs annually.35,36
Although folic acid fortification is a productive method for increasing serum folate concentration among women of reproductive age and should be continued in the US, it is insufficient as the sole source of folate for pregnant individuals. The average US adult consumes 140 µg of folic acid from foods under the enrichment specification, far below the WHO 400-µg recommendation for pregnant individuals.16,37 The multifaceted public health strategy employed by the Centers for Disease Control, coupling mandatory food fortification and supplement recommendations by clinicians, prevents an additional 700 NTDs annually.35A combination approach is the ultimately the best way to ensure pregnant mothers maintain a healthy folic acid level. Thus, it is critical that mothers have access to proper prenatal supplements and folic acid enriched foods.
Barriers to Folic Acid Supplementation Efforts
Although folic acid supplementation is well established as a critical piece of prenatal care, many countries struggle to achieve adequate coverage of supplement delivery to their pregnant population. A comprehensive, mixed-methods analysis conducted in Afghanistan, Bangladesh, Indonesia, Ethiopia, Kenya, Nigeria, and Senegal analyzed the barriers and enablers to prenatal supplementation rates.38 All countries studied had national policies in place for prenatal supplementation; however, the degree of coverage varied based on the breadth of each program and the types of strategies used. Accessibility, both geographic and financial, was the most common external barrier to supplementation coverage. Even with subsidized supplements, pregnant individuals still reported financial barriers, noting the cost of prenatal care visits as hindering their access.38 Other common obstacles include gaps in clinician training, low perceived value for prenatal care, fear of the medical system, a lack of community interventions, and skepticism over the legitimacy of community providers.38 Future population-based public health initiatives should target these issues to best address the population’s needs.
Even when pregnant individuals receive prenatal supplements, the priority they place on adherence to the supplement regimen still limits the overall coverage of folic acid supplement consumption. Medication adherence is one of the most significant challenges clinicians face during public health initiatives.39 Currently, there is no extended-release folic acid supplement available on the market; thus, daily supplementation is required to maintain adequate levels. A global, systematic review of prenatal adherence initiatives found that education-based interventions are the most common and effective way to improve adherence to nutrient supplementation during pregnancy.40 Specifically, one of the most influential enablers of prenatal supplementation adherence is a thorough education on maternal anemia with an emphasis on the physiologic causes and methods for prevention.38 More extensive research is required to develop a comprehensive view of other protocols’ efficacy in targeting adherence.
Future Directions
Current trends in prenatal supplementation research advocate for the use of 5-MTHF in place of folic acid in commercial prenatal supplements. Folic acid has no biological function and cannot be metabolized until dihydrofolate reductase reduces it, yet 5-MTHF is available for metabolism and transport immediately following consumption, thus increasing its bioavailability.41 The push for this shift stems from the elevated prevalence of genetic polymorphisms that affect folic acid metabolism among specific demographic populations, which could account for the lower serum folate levels and the higher rate of NTDs in the Hispanic population.36 Retrospective research has also shown a statistically significant reduction in preeclampsia incidence among mothers who began taking 5-MTHF during their first trimester.42 Concerns over masking the symptoms of vitamin B12 deficiency and the development of megaloblastic anemia are also mitigated when replacing folic acid supplements with 5-MTHF.43 Furthermore, the use of 5-MTHF eliminates the risks associated with excess UMFA levels because it bypasses folic acid metabolism.3 Although research advocates for the benefits of 5-MTHF over folic acid supplementation, the commercial prenatal supplementation industry has yet to transition from folic acid to 5-MTHF. The current standard of care recommends folic acid supplementation, a choice supported by folic acid’s increased heat stability and lower cost.43 As of 2022, 71% of commercial supplements contain exclusively folic acid, 15% contain exclusively 5-MTHF, and 13% contain a combination of the 2.3 The Table provides the advantages and disadvantages of both folic acid and 5-MTHF supplements. Given the updated research, researchers expect that 5-MTHF supplementation will be integrated into prenatal vitamins in place of folic acid.2,3,44 Most of the challenges with 5-MTHF are related to its novelty in the prenatal supplementation space, but its use and integration into the standard of care for prenatal health in the future remains possible as familiarity grows and more extensive research is conducted. Based on the existing literature and several prenatal complications avoided when using 5-MTHF, more manufacturers are urged to consider developing these 5-MTHF–rich supplements and physicians to integrate them into their recommendations for prenatal care.
Conclusions
This robust volume of evidence strongly links folate levels to embryologic development and maternal and fetal health.3 Although the specific mechanism remains unknown, the flux of folate through the folate and 1-carbon cycles is directly involved in homocysteine methylation and nucleic acid synthesis. The role of folate in DNA methylation and epigenetic regulation provides a direction for future research to explore the physiologic basis of folate’s critical role in embryonic neural development. Furthermore, several studies have identified target genes contributing to NTDs, providing another clear avenue for further research. The scientific community largely believes that new research in the genetic sphere with Shh and Sufu can give a more comprehensive understanding of NTDs, which will, in turn, guide clinical practice and recommendations. Despite the ambiguity surrounding the direct mechanism, the relationship between folate deficiencies and NTDs is well established, indicating that folic acid supplementation remains an essential part of the standard of care for prenatal vitamin complexes. Current public health strategies include international recommendations for supplemental folic acid consumption among women of reproductive age, accompanied by mandatory dietary fortification in some countries. The mechanistic advantage of 5-MTHF supplementation in place of traditional folic acid may further improve the already strong impact of folate supplements, and our research predicts a shift in supplementation trends towards 5-MTHF in the future. On reviewing the existing guidelines relative to population incidence rates, it seems that population-based efforts effectively reduce fetal birth defects and are a necessary step for all countries to improve maternal and infant health.
Conflict of Interest
All authors have no conflicts to disclose.