Introduction
Tendinopathies are a group of conditions defined by pain and dysfunction in the tendons, commonly resulting from overuse or degeneration.1 They are a significant source of musculoskeletal pain, affecting various parts of the body, including the shoulders, elbows, and hips. Tendinopathies can severely impact an individual’s quality of life and ability to perform daily activities or sports. The pathophysiology of tendinopathies involves complex changes at the anatomical and cellular levels, and is crucial to understand for effective treatment and management. Tendons are robust connective tissues that attach muscles to bones, transmitting the force generated by muscles to facilitate movement. They are composed primarily of collagen fibers, proteoglycans, and water organized into a hierarchical structure that provides tensile strength and flexibility. Tendinopathies occur when this structure is compromised, often due to repetitive mechanical loading or acute trauma. On an anatomical level, tendinopathies are characterized by collagen disarray, increased ground substance, and neovascularization. These changes result in decreased tensile strength and increased susceptibility to injury.
There are several types of tendinopathies, with rotator cuff tendinopathy, lateral epicondylitis (tennis elbow), and gluteal tendinopathy being among the most common. Rotator cuff tendinopathy affects approximately 22% of the general population, with prevalence increasing with age.2 Lateral epicondylitis affects about 1% to 3% of adults annually in the UK, especially those aged between 40 and 49 years.3 Gluteal tendinopathy is estimated to affect 25% of women older than 50 years.4 Rotator cuff tendinopathy affects the tendons of the rotator cuff muscles in the shoulder, leading to pain and restricted movement. It is most common in athletes and individuals engaged in repetitive overhead activities.5 Lateral epicondylitis affects the tendons on the outer side of the elbow, commonly seen in tennis players, golfers, and those working in occupations requiring repetitive wrist and arm movements. Gluteal tendinopathy involves the tendons of the gluteus medius and minimus muscles in the hip, causing pain and difficulty in movements such as walking and climbing stairs. The main symptoms of tendinopathies include localized pain, tenderness, and impaired function of the affected tendon. The affected area may exhibit swelling, warmth, and decreased range of motion, significantly impacting daily activities and athletic performance.
Current treatment modalities for tendinopathies include conservative approaches such as physical therapy, nonsteroidal anti-inflammatory drugs, and corticosteroid injections. Physical therapy is a cornerstone of tendinopathy management, focusing on exercises that improve flexibility, strength, and proprioception of the affected tendon and surrounding muscles.6 This involves a range of exercises tailored to the specific tendinopathy, including eccentric loading exercises, stretching, and manual therapy. Outcomes of these interventions are typically assessed using validated scoring systems, including the visual analog scale (VAS) for pain, American Shoulder and Elbow Surgeons (ASES) score for shoulder function, and Western Ontario Rotator Cuff (WORC) index, among others. These tools help quantify pain relief and functional improvement over time. Nonsteroidal anti-inflammatory drugs help manage pain and inflammation associated with tendinopathies; however, their use is typically limited to short-term relief due to potential adverse effects with prolonged use. Corticosteroid injections are widely used for their anti-inflammatory and pain-relieving properties, but they often provide only short-term relief and can be associated with adverse effects such as tendon degeneration and recurrence of symptoms.
Platelet-rich plasma (PRP) therapy has emerged as a potential alternative treatment for tendinopathies. PRP is an autologous blood product rich in platelets and growth factors, which may promote tissue repair and regeneration.7 PRP therapy involves injecting concentrated platelets directly into the affected tendon, aiming to enhance the healing process and provide longer-lasting relief from symptoms. PRP therapy has shown promise in treating a variety of musculoskeletal conditions beyond tendinopathies. It has been used successfully in the management of osteoarthritis, particularly in the knee, where it helps in reducing pain and improving joint function. PRP has also been used in the treatment of acute muscle injuries, ligament sprains, and cartilage defects, showing positive outcomes in accelerating recovery and improving tissue quality. Additionally, PRP has been applied in plastic surgery, dermatology, and wound healing, where its regenerative properties contribute to improved healing and aesthetic results.8
The goal of this systematic review was to compare the efficacy of PRP and corticosteroid injections in the treatment of various tendinopathies. Specifically, this review is focused on rotator cuff tendinopathy, lateral epicondylitis, and gluteal tendinopathy. By analyzing the outcomes of multiple randomized clinical trials (RCTs), this review aimed to determine whether PRP therapy offers superior pain relief and functional improvement compared with corticosteroid injections and to evaluate the long-term vs short-term benefits of both treatments.
Methods
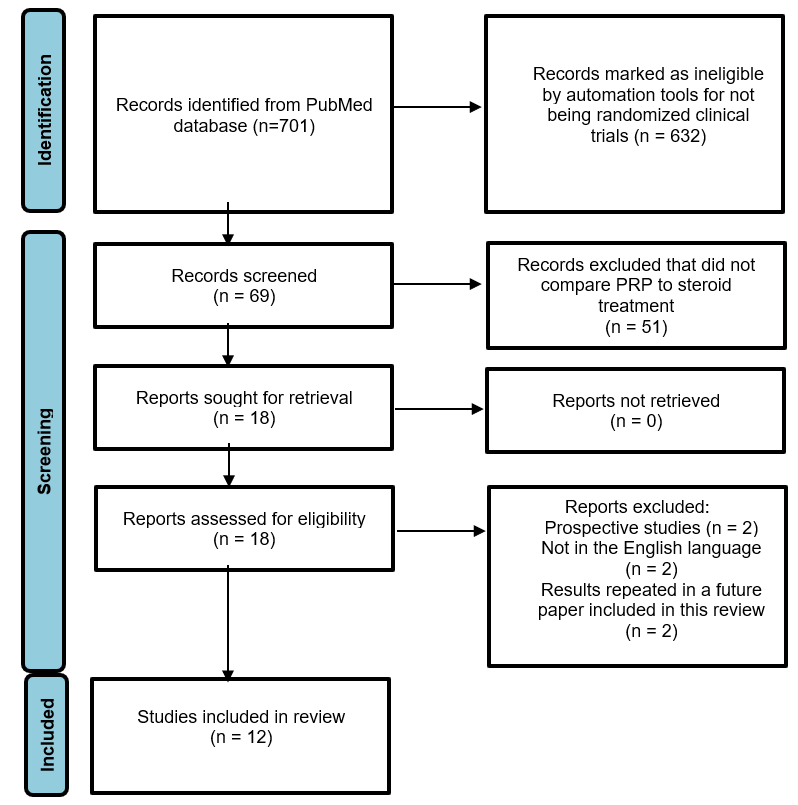
The systematic review was conducted using the PRISMA guidelines and included a literature search conducted using only the PubMed database. The literature search was conducted in July 2024 using the following terms: platelet-rich plasma and tendinopathies. Studies that were not RCTs or were prospective studies were excluded from this review. Articles that did not specifically compare the efficacy of PRP vs steroids were excluded from the review. Only articles in the English language were included. An ethics committee was neither involved nor required in this systematic review. The initial search and screening were performed by K.M. and independently reviewed by Y.J. and R.R. From each study, the following data were extracted: type of tendinopathy, study design, sample size, interventions used, duration of follow-up, and outcome measures. Clinical outcomes included pain scores (eg, VAS), functional scores (eg, ASES and WORC), treatment failure or recurrence rates, and any reported adverse effects related to PRP or corticosteroid injections. The Figure highlights the PubMed literature search process.

Results
A total of 13 RCTs were included, evaluating the efficacy of PRP vs corticosteroid injections in the treatment of 3 tendinopathies: rotator cuff tendinopathy,9–13 lateral epicondylitis,14–18 and gluteal tendinopathy.19,20 Study populations primarily included adults with chronic tendinopathy who had not responded to prior conservative treatment. PRP formulations varied, including both standard and leukocyte-rich preparations, and corticosteroid injections most commonly involved triamcinolone. Outcomes were assessed using validated tools such as the VAS for pain; the ASES score; the WORC index; the Disabilities of the Arm, Shoulder, and Hand (DASH) score, the Constant-Murley Score (CMS), and the modified Harris Hip Score (mHHS), among others. The Table summarizes study characteristics, treatment protocols, follow-up durations, and results.
Rotator Cuff Tendinopathies
Five studies9–13 assessed PRP vs corticosteroids in rotator cuff–related conditions, including shoulder impingement syndrome, partial thickness tears, and calcific tendinitis. Most studies reported greater improvements in PRP-treated groups, particularly at mid- to long-term follow-ups (3-12 months). Functional scores such as ASES, WORC, and CMS improved significantly more in the PRP group in 4 of the 5 studies.10–13 One study reported significantly better shoulder abduction at 1-year follow-up in the PRP group, despite similar short-term pain scores.11 In contrast, corticosteroids were more effective at short-term pain relief (eg, at 1 week), but this benefit did not persist in most studies.
Lateral Epicondylitis
Five RCTs14–18 evaluated PRP vs corticosteroids for lateral epicondylitis. All studies showed improvement in both treatment groups; however, 4 of 5 found that PRP produced more sustained relief in pain and function at 6 to 12 months.14,16–18 Corticosteroids typically offered rapid improvement in symptoms at 2 to 6 weeks but was associated with higher recurrence rates. One study also reported signs of tendon degeneration in the corticosteroid group on follow-up imaging.21 VAS and DASH scores consistently improved in the PRP group across all time points in several studies, particularly beyond 3 months.
Gluteal Tendinopathy
Two studies19,20 compared PRP and corticosteroids in the treatment of chronic gluteal tendinopathy. Both demonstrated that PRP led to significant improvements in pain and function, measured by mHHS and VAS, particularly over longer follow-up periods (up to 104 weeks). In the crossover design used by Smidt et al,22 patients for whom corticosteroid treatment did not initially work improved significantly after switching to PRP. Magnetic resonance imaging findings also showed structural tendon improvements, including increased tendon thickness, in the PRP group.23
Overall Synthesis
Among the 12 studies included, 10 reported superior long-term outcomes with PRP in at least 1 major clinical outcome compared with corticosteroids.10–20 Corticosteroid injections showed faster pain relief in the short-term (≤6 weeks) in 5 studies, but were often associated with symptom recurrence or diminishing effects over time.10,12,13,15,19 Adverse events were minimal across all studies. Only 1 study reported imaging evidence of tendon degeneration in corticosteroid-treated patients.15 Reintervention rates were lower in PRP-treated patients, especially in crossover or extended follow-up trials. Collectively, the evidence supports use of PRP as a potentially more durable treatment option across multiple types of tendinopathies.
Discussion
Rotator Cuff Tendinopathies
This review analyzed 5 studies that compared the efficacy of PRP treatment vs corticosteroid treatment in reducing pain and improving function in patients with rotator cuff tendinopathy.9–13 The RCTs reviewed in this article suggest that PRP treatment improves pain more significantly compared with corticosteroid treatment at the 3-month or 6-month follow-ups from baseline as measured by the VAS or numeric rating scale.9–13 However, no significant difference in pain was observed between PRP and CS at 6-week or 12-month follow-up periods in any of the studies. In terms of functional outcomes, most studies showed significantly greater improvements in the PRP group at the 3-month follow-up as well.11,12,24 Function was measured by range of motion, ASES score, WORC score, Simple Shoulder Test, and CMS. However, the study by Hewavithana et al.9 did show significant differences in range of motion in favor of the PRP group at the 12-month follow-up. Only the Oudelaar et al.12 study showed a significant improvement in functional outcome in the corticosteroid group compared with the PRP group at the 6-week follow-up as measured by CMS, the DASH score, Oxford Shoulder Score, and EuroQol 5-Dimension score. The corticosteroid group also showed significant improvement compared with the PRP group in the EuroQol 5-Dimension score at the 3-month and 12-month follow-ups. This discrepancy in study results may be attributed to treatment differences; the Oudelaar et al12 study involved a PRP or corticosteroid treatment after patients underwent needle aspiration of calcific deposits (NACD). This suggests that corticosteroid injections may improve function more than PRP when administered after NACD treatment. Overall, these results suggest that PRP treatment leads to greater improvement in pain and function compared with corticosteroid treatment in patients with rotator cuff tendinopathy in the shorter-term (approximately 3 months post injection), but this effect is not sustained in the long-term (approximately 6 months and 12 months post injection). Rotator cuff tendinopathy is one of the more common causes of shoulder pain, with approximately 30% of the general population experiencing it.10 Corticosteroid injections have been used as a nonoperative treatment for a wide range of shoulder disorders, but recent studies have suggested that they might be responsible for playing a possible deleterious role, decreasing the rotator cuff tendon quality and increasing the need for revision of rotator cuff repair.21,25–29 With few cases of adverse events reported with PRP treatment, it proves to be a more effective treatment modality, especially for the short-term. However, PRP treatment has shown greater long-term efficacy than corticosteroids in the treatment of other pathologies, such as knee osteoarthritis, sacroiliac arthropathy, plantar fasciitis, and greater trochanteric pain syndrome.16,21 The shorter-term efficacy of PRP over corticosteroids may be applicable more to shoulder lesions specifically.
Lateral Epicondylitis
This review also compared the efficacy of PRP treatment vs corticosteroids in patients with lateral epicondylitis. The RCTs reviewed in this article suggest that PRP improves pain relief more significantly than corticosteroids approximately 1 month after injection and up to 2 years.14–18 The corticosteroid group showed significant improvements in pain relief compared with PRP in the period between the injection and the 1-month follow-up. Pain improvement was measured using the VAS. In terms of functional outcome overall, most studies showed more significant improvement in the corticosteroid group compared with the PRP group up to 6 weeks post injection, after which PRP showed significantly greater functional outcomes up until 2 years in some studies.14–18 Some of the measures included DASH, modified Mayo score, Mayo Elbow Performance Score, or Global Symptom Score. Overall, this suggested that corticosteroids may be more effective in reducing and improving outcomes of patients with lateral epicondylitis in the shorter-term, but PRP may have a more sustained effect lasting up to 2 years post injection. This is, in fact, the opposite of what was observed for rotator cuff tendinopathy that showed PRP to be more efficacious compared with corticosteroids in the short-term, but not the longer-term.9–13 However, as with rotator cuff tendinopathies, corticosteroids have been a long-time standard invasive treatment for lateral epicondylitis and comes with similar problems of high relapse and recurrence rates. This could be attributed to the fact that the intratendinous corticosteroid injections may lead to adverse effects to the structure of the tendon itself.22 The longer-term effect of PRP over corticosteroids may be due to the long-lasting effects of platelets in the PRP that specifically improve very early on in the repair of neotendon properties, so cells respond to mechanical loading early in the repair process.23 There is an ongoing debate about the improved results of more than 1 PRP injection being used to treat lateral epicondylitis. All the studies included in this review only gave 1 injection of PRP, which resulted in long-term improvements. Future studies should compare 2-injection PRP vs corticosteroids to observe whether PRP shows more significant improvement in the short-term too.
Gluteal Tendinopathies
This review also analyzed the efficacy of PRP compared with steroid in the treatment of gluteal tendinopathies, one of the more common reasons for hip and buttock pain. The 2 studies reviewed in this article suggested that the PRP group showed better pain and function outcomes compared with the corticosteroid group between 3 months and 1 year post injection, but not significantly different before 3 months after the injection.19,20 This was measured by VAS and mHHS. This suggests that, similar to lateral epicondylitis and different than rotator cuff tendinopathies, PRP is more effective than corticosteroids as a treatment in the short-term. However, PRP is also shown to be noninferior to corticosteroids in the short-term (<3 months post injection). Also, as observed in the Carney and Fitzpatrick study,20 there were structural improvements seen in the PRP group that were not observed in the steroid group.19 This suggests that PRP may actually aid in reversing the degenerative structural changes of the tendons. The type of PRP injections used has been controversial. The Fitzpatrick et al.19 study used leukocyte-rich PRP and showed effective results. The varying levels of platelets and white blood cells in different types of PRP can affect the efficacy of the injection in improving pain and outcomes in gluteal tendinopathies.
Failure Rates and Adverse Effects
Along with analyzing the differences in efficacy of PRP compared with corticosteroids in treating tendinopathies, it is also important to note the differences in failure rates or adverse effects. Most of the rotator cuff tendinopathy studies reviewed in this article suggested a similar rate of failure of treatment when using PRP injection compared with corticosteroid injection, showing no serious adverse events.9,10 The Oudelaar et al.12 study did suggest more complications in the NACD plus PRP group (5 frozen shoulders, 1 chemical bursitis) compared with the NACD plus corticosteroids group (1 chemical bursitis). However, this difference did not affect pain and functional scores at the 2-year follow-up. Moreover, a significantly greater proportion of the corticosteroids group required a second NACD treatment compared with the PRP group. The lateral epicondylitis studies reviewed also suggested no serious adverse events in either the PRP or corticosteroid treatment groups. According to the Krogh et al16 and Gosens et al.17 studies, more people reported persistent pain in the PRP group vs the corticosteroid group, but that may be due to the PRP treatment activating the inflammation cycle initially. In regard to the need for reintervention, Gosens et al.17 and Peerbooms et al.18 showed more reinterventions in the corticosteroid group compared with the PRP group. Fitzpatrick et al.19 also suggested there were no serious adverse events for the corticosteroid and PRP groups among patients with gluteal tendinopathy. Overall, the studies reviewed suggested there were no serious adverse effects noticed for either PRP or corticosteroid injections. However, it was noticed that corticosteroid injections required more reinterventions and the PRP group reported more persistent pain than the corticosteroid group. However, it is important to consider some of the potential complications associated with long-term use of corticosteroids for tendinopathies. Corticosteroid usage carries the risk of local skin complications, such as rash and hypopigmentation, along with major adverse events, such as atrophy, cellulitis, and calcification.20 Corticosteroid injections can also lead to further tendon structural damage, such as tendon weakening and ruptures with repeated injections of corticosteroids.20 Comparatively, PRP is known to have fewer, less serious complications, including temporary pain, bruising, and skin irritation at the site of the injection. This suggests PRP injection to be favored over the corticosteroid injection for tendinopathy treatment, especially due to PRP’s more sustained, long-term effectiveness.
Cost-Benefit Analysis of PRP Compared With Corticosteroids
A study using Markov modeling to evaluate the cost-effectiveness of PRP compared with corticosteroids for recalcitrant lateral epicondylitis found that both treatments were cost-effective under a willingness-to-pay threshold of $50 000 per quality-adjusted life-year (QALY). However, PRP was found to be the dominant strategy, meaning it was more cost-effective than corticosteroids, with lower costs and higher effectiveness.30 Specifically, PRP had an incremental cost-effectiveness ratio of –$5846.97/QALY from a health care perspective and –$9392.33/QALY from a societal perspective, indicating that it not only provided better health outcomes, but also saved money compared with corticosteroids. The net monetary benefit further supported the superiority of PRP. From a health care perspective, PRP injections provided a net monetary benefit of $217 863.98, while corticosteroids provided $197 534.18.30 From a societal perspective, PRP also had a higher net monetary benefit ($214 820.16) compared with corticosteroids ($193 199.75). This reinforces that PRP offers a higher value for the investment when considering both direct health care costs and broader societal impacts.
Conclusions
Overall, the studies reviewed here suggested that PRP is more effective than corticosteroids in reducing pain and improving function in the short-term for rotator cuff tendinopathies, but in the longterm for lateral epicondylitis and gluteal tendinopathies. Corticosteroids also showed some structural deterioration of the tendons in some of the studies, which was not seen in the PRP group. The studies also showed no serious adverse events for either treatments, but the corticosteroid groups did require more reinterventions and the PRP groups did have more persistent pain initially. The more serious long-term adverse effects of corticosteroid usage and the increased efficacy of PRP vs corticosteroids may suggest that the use of PRP is preferable corticosteroids in the management of tendinopathies. Future research should focus on the economic analysis of PRP vs corticosteroids, comparing the cost-effectiveness of the treatments in tendinopathy management. In addition, future studies should focus on comparing the efficacy of leukocyte-rich PRP and leukocyte-poor PRP in the treatment of tendinopathies.
Conflicts of Interest
The authors declare that they have no conflict of interests.