Introduction
Tianeptine, often referred to as Zaza, Red, and Tianaa, has gained attention in recent years due to its unique pharmacological properties and increasing use both medically and recreationally.1 Developed in the 1980s as an atypical tricyclic antidepressant, tianeptine was approved in parts of Europe, Asia, and Latin America for the treatment of major depressive disorder, dysthymia, and, in some cases, anxiety and irritable bowel syndrome.1,2 Despite its international use under brand names like Coaxil, Stablon, and Tatinol, the US Food and Drug Administration has not approved tianeptine, citing concerns about its abuse potential and limited data supporting its safety and efficacy.1,2
Against the backdrop of a national opioid crisis, tianeptine’s full agonist activity at the µ-opioid receptor, similar to classic opioids, underlies its addictive properties and raises alarms to its potential misuse. Tianeptine exerts its antidepressant effects primarily through modulation of the glutamatergic system, enhancing glutamate transmission by increasing the reuptake of serotonin (5-hydroxytryptamine) in contrast to selective serotonin reuptake inhibitors, which inhibit serotonin reuptake.3,4 Furthermore, tianepatine has been shown to regulate dopamine release, with additional evidence suggesting that it may have anti-inflammatory effects via microglial suppression.3,4 Tianeptine has a short half-life of approximately 2.5 hours and is metabolized via β-oxidation into two principal metabolites, MC3 and MC5. MC3 is considered to have minimal pharmacologic activity and is not thought to contribute significantly to the drug’s clinical effects, whereas MC5 is the primary active metabolite in plasma and exhibits modest antidepressant and μ-opioid receptor activity.5 In elderly individuals, MC5 has a terminal half-life of 11.9 ± 8.0 hours and low renal clearance (3.1 ± 2.3 mL/min), which contributes to prolonged systemic effects.6
In recent years, reported tianeptine human exposure or cases documented in poison center data have increased substantially, with an approximate 1400% rise between 2015 and 2023. In the United States, tianeptine is increasingly accessible through online vendors and retail outlets, including convenience stores and gas stations, and is often marketed as a dietary supplement, which does not require premarket approval by the US Food and Drug Administration.7 This increased availability may have contributed to the rising number of reported exposures. Reports of withdrawal symptoms, dependency, and overdose cases have surfaced, prompting further investigation into its patterns of use, particularly in the United States.1,8 A rat model study (2022) demonstrated motor impairment, gastrointestinal hypomotility (including constipation), and respiratory depression, primarily at higher or supratherapeutic doses, consistent with μ-opioid receptor–mediated effects.9 These effects were mirrored in a retrospective review of calls received by a poison control center in cases where tianeptine was identified as an agent of intoxication. Lethargy was the most common sign at presentation, with agitation, gastrointestinal distress, and anxiety being common symptoms of withdrawal. Recent findings demonstrate a statistically significant rise in tianeptine exposure over time, suggesting increasing detection or utilization within healthcare systems. More than half of the 48 cases reviewed led to hospital admission, and 35% of cases studied escalated to admission to an intensive care unit.10 Public concerns over tianeptine have led to sales restrictions in eight states, including Alabama, Georgia, Indiana, Kentucky, Michigan, Mississippi, Ohio, and Tennessee.11
Despite mounting concern, large-scale epidemiologic data on tianeptine use in the United States are limited. This study seeks to address that gap by analyzing tianeptine-related trends using electronic health record (EHR) data from the TriNetX Global Collaborative Network. Findings may inform clinical guidance, regulatory action, and public health responses aimed at mitigating the risks associated with tianeptine misuse.
Methods
Study Design and Data Source
We conducted a retrospective cohort study using de-identified EHR data from the TriNetX Global Collaborative Network, encompassing 129,740,865 patients across 129 healthcare organizations. The network primarily includes US-based data with additional international contributions (eg, Europe, Asia); however, site-level geographic details are not available due to de-identification. The study period spanned January 1, 2010, to December 31, 2024, and was divided into two intervals (2010-2017 and 2018-2024) to evaluate temporal trends before and after the rise in reported tianeptine exposures in the late 2010s. The primary objective was to assess the incidence and prevalence of tianeptine-related encounters, stratified by age, sex, race, and ethnicity. Patients were identified using documented drug name entries (eg, Zaza, Zaza Red, tianeptine, Tianaa) within clinical encounter or prescription records.
Data Analysis
Processing and data extraction were conducted using the TriNetX web-based research platform (TriNetX, Cambridge, Massachusetts), utilizing the Global Collaborative Network comprising 141 healthcare organizations and 129,740,865 patients. Summary data were exported into Python (version 3.11) for statistical analysis using the pandas and statsmodels packages (version 0.14.0). The analysis was stratified across two time periods: January 1, 2010, to December 31, 2017 (pre-period), and January 1, 2018, to December 31, 2024 (post-period). Incidence proportions and prevalence were calculated as the number of unique patients with a record of tianeptine use divided by the total number of patients within each period, expressed as cases per 100,000 individuals and per 100,000 person-days, respectively, with absolute case counts derived from these proportions. Projected incidence rates for 2025-2030 were estimated using linear extrapolation based on observed trends between the two study periods (2010-2017 and 2018-2024), assuming a continuation of the existing trajectory. A 2×2 contingency table was constructed to compare tianeptine cases and noncases between time periods; due to low event rates, statistical significance was assessed using the Fisher exact test, with additional confirmation using a {}2 test for independence. Effect sizes were reported as relative risk and odds ratio with corresponding 95% confidence intervals. Missing or unspecified demographic values (eg, “Unknown Race”) were retained as separate categories to preserve sample size. Statistical significance was defined as a 2-sided P<.05.
Ethical Considerations
The data reviewed is a secondary analysis of existing deidentified data, does not involve intervention or interaction with human subjects, and is deidentified according to the de-identification standard defined in the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. This retrospective study is exempt from informed consent and from institutional review board approval in accordance with the HIPAA Privacy Rule.
Results
Primary Outcome: Significant Increase in Incidence
Between the study periods of 2010-2017 and 2018-2024, there was a significant increase in the incidence of tianeptine-related encounters across the TriNetX Global Collaborative Network. The incidence proportion increased from 0.58 to 4.30 cases per 100,000 individuals, corresponding to an odds ratio of 7.54 (P<.001, Fisher exact test). The relative risk was also 7.54, indicating a 7.5-fold higher likelihood of tianeptine-related encounters in the later period compared with the earlier period. Similarly, incidence proportion and prevalence increased from 0.06 to 0.43 cases per 100,000 individuals between the two timeframes. In the later period (2018-2024), the incidence proportion was 4.30 cases per 100,000, prevalence was 4.60 cases per 100,000, and the incidence rate was 0.43 cases per 100,000 person-days. These findings suggest a notable rise in tianeptine detection, potentially owing to increased use or improved detection methods.
Age-Specific Trends
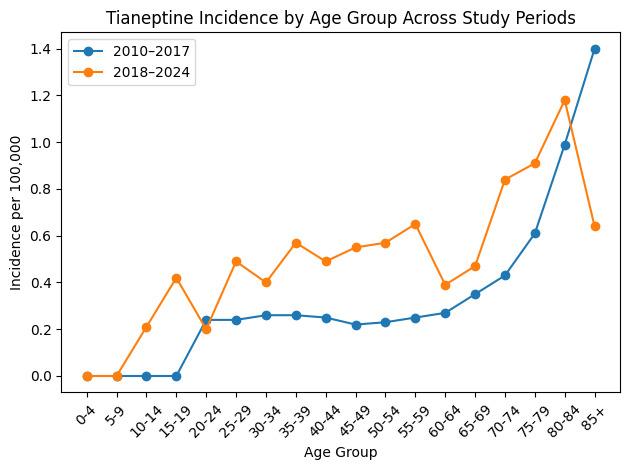
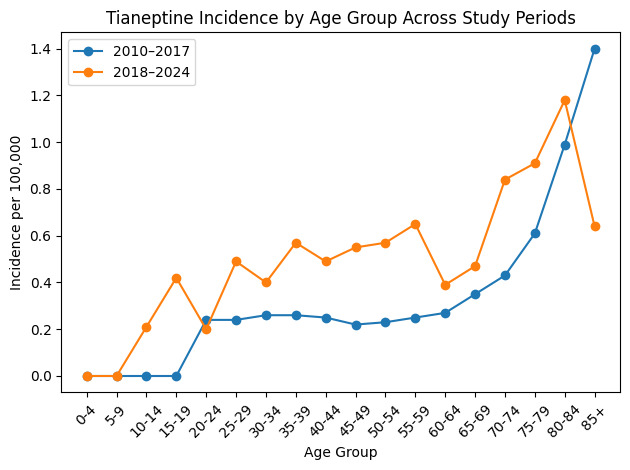
Age-specific trends revealed important shifts in the affected populations. During the 2010-2017 period, no cases were identified in individuals younger than 20 years (Table 1). Incidence began in the age group 20 to 24 years old and increased progressively with age, with the highest rates occurring in those 85 years and older (1.40 cases per 100,000 individuals). In contrast, during the 2018-2024 period, tianeptine cases began appearing in younger demographics, including the age groups 10 to 14 years old and 15 to 19 years old. Meanwhile, the highest incidence shifted to the age group 70 to 79 years, and detection rates among the population 85 years and older declined.
In the 70- to 74-year-old age group, cases nearly doubled, from 0.43 to 0.84 per 100,000. The 75- to 79-year-old age group saw a 50% increase, from 0.61 to 0.91 per 100,000, while the 80 to 84 years old age group experienced a more modest rise of 19%, from 0.99 to 1.18 per 100,000. Higher incidence was observed among younger elderly populations, while a decline was noted in the 85 years and older age group. If current trends persist, incidence may continue to shift toward younger age groups. Age-specific incidence trends across the two study periods are illustrated in Figure 1.
Incidence by Race and Sex
Tianeptine incidence by sex revealed notable differences between males and females across time periods. From 2010 to 2017, females exhibited a higher incidence rate (0.08 cases per 100,000) compared with males (0.04 cases per 100,000). This pattern persisted in the 2018-2024 period, with incidence rates increasing to 0.54 per 100,000 in females and 0.33 per 100,000 in males. Time trend analysis indicated a 14% increase in incidence among females, while male incidence declined by 15% during the same period.
During the 2010-2017 period, no cases were detected among Black populations. The highest incidence was observed in the “Other Race” category (0.28 cases per 100,000) followed by the “Unknown Race” category (0.16 cases per 100,000). White patients had comparatively lower incidence rates (0.03 per 100,000). During the 2018-2024 period, Black individuals exhibited an incidence rate of 0.12 per 100,000, while White individuals in the same period showed a decline to 0.008 per 100,000. During the period 2010-2017, White males and females had incidence rates of 0.32 and 0.76 per 100,000, respectively.
In the 2018-2024 period, incidence declined in both groups to 0.24 per 100,000 in White males and 0.54 per 100,000 in White females. In contrast, new cases emerged among Black individuals, with incidence reaching 0.33 per 100,000 in Black males and 0.87 per 100,000 in Black females. Projections for 2025-2030 indicate a continued shift: Black females are expected to have the highest incidence (0.92 per 100,000) followed by White females (0.59), Black males (0.38), and White males (0.29). These findings indicate changes in demographic patterns of tianeptine-related incidence, with higher rates observed among Black populations, particularly females.
During the period 2018-2024, Black females aged 70 to 84 years had an incidence of 0.90 cases per 100,000, representing the highest rate among elderly subgroups. Among young adults aged 20 to 24 years, Black females also exhibited the highest incidence (0.87 cases per 100,000) compared with other demographic groups in that age range. Projected estimates for 2025-2030 indicate similar patterns, with incidence rates of 0.91 per 100,000 in the elderly population and 0.88 per 100,000 among young adults.
Discussion
With an ongoing US opioid epidemic, growing trends involving drugs with opioid-like effects, such as tianeptine, raise serious public health concerns and safety issues. Comparative analysis between the periods 2010-2017 and 2018-2024 demonstrated a decline in tianeptine-related incidence among White individuals across all age groups and genders—notably, with a 25% decrease in White males and a 29% decrease in White females. These shifts may reflect differences in accessibility, widespread nonprescription availability, and evolving patterns of use, as well as potential variation in detection or reporting across demographic groups. Among elderly populations (aged 70-84 years), Black females experienced a 125% increase in cases, overtaking White individuals who previously exhibited the highest incidence.
These shifts suggest changes in prescribing patterns, accessibility, or emerging use trends in different racial groups.12,13 Notably, our findings diverge from prior studies that documented tianeptine-involved emergency department visits in Tennessee (2021-2023), which identified non-Hispanic White males as the most frequent demographic to visit.14 Historically, opioid abuse has been framed as a “White” issue, often overshadowing the experiences of other racial groups.15 This framing is partly reinforced by research showing that Black individuals are less likely to be prescribed opioids due to racial bias regarding pain tolerance.16 However, the increasing availability of tianeptine through unregulated sources (online vendors and gas stations) may be altering patterns of access and misuse, particularly among underserved populations.
While literature on tianeptine misuse is sparse, opioid-related studies offer valuable context. Opioid exposures have driven increasing hospitalization rates among adolescents and young adults. A longitudinal study tracking individuals aged 13 to 25 years from 2001 to 2014 found a 6-fold increase in new diagnoses of opioid use disorder.17 Additionally, early exposure to opioids before high school graduation was associated with a 33% increased risk of future misuse.18 Our findings suggest that tianeptine exposure and subsequent misuse may be following a similar pattern. The emergence of tianeptine-related cases among young adults, particularly among Black females aged 20 to 24 years, suggests a potential shift in exposure patterns within younger populations. Similar emerging trends among Black males further support changing demographic patterns over time.
These trends highlight a troubling expansion of tianeptine use among young populations, potentially driven by increased recreational use, self-medication, or changes in awareness and screening. The literature remains inconclusive regarding gender differences in misuse: some reviews report men accounting for 76% of tianeptine misuse cases, whereas other studies cite women accounting for 75% of cases.19 However, one study reported that 77% of tianeptine misuse cases involved individuals 35 years or younger.20 Given the drug’s unregulated status and ease of access, risk of misuse among youth is especially concerning and underscores the need for targeted interventions.
The intersection of race and gender, especially in the case of Black women, has long been associated with compounded systemic barriers to accessing substance use treatment.21 As seen in Table 2, incidence among Black females aged 70 to 84 years rose to 0.90 per 100,000, surpassing all other elderly subgroups. If current trends persist, Black females across both young adult and elderly populations may remain the most at-risk demographic for tianeptine exposure and toxic effects. Predictive modeling indicates that incidence rates in this group are likely to continue rising, while rates among White populations are expected to decline. This pattern highlights the need for targeted public health interventions that focus on Black females aged 20 to 24 years and 70 to 84 years.
The observed demographic differences in tianeptine-related incidence are not fully explained by known pharmacologic mechanisms. Tianeptine is primarily metabolized through β-oxidation of its heptanoic side chain.22 Although some studies suggest that women may exhibit higher levels of β-oxidation enzymes compared with men, there is no evidence demonstrating significant variation in β-oxidation capacity across racial or ethnic groups.23,24 These findings suggest that pharmacokinetic differences alone are unlikely to account for the higher incidence observed among Black females, indicating that other factors may contribute to the observed disparities.
As detailed in Table 1, the highest incidence in the earlier study period occurred among the oldest adults (>85 years), but by 2018-2024, rates had shifted toward slightly younger elderly populations. Age-related changes in β-oxidation have been documented, often contributing to dysregulated lipid metabolism in older adults.25 This may help account for the rising incidence of tianeptine use with age. Unlike many antidepressants, tianeptine is not metabolized by the hepatic cytochrome P450 system, minimizing drug-drug interactions, which are of particular interest when treating elderly patients with depression.5 An international study found that an 8-week course of 25 to 50 mg of tianeptine was effective for treating depression in patients 65 years and older.26 However, standard clinical guidelines recommend initiating antidepressant therapy at lower doses in older adults, underscoring the risks associated with the unsupervised use of substances like tianeptine that have not been approved by the US Food and Drug Administration.27
Clinical Implications
Although the literature on tianeptine misuse remains limited, the disproportionate burden observed among Black women reflects broader trends in opioid use. Since 2013, the opioid overdose mortality rate has increased significantly in the Black population, primarily due to synthetic opioids.28 These parallels highlight the urgent need for further research into tianeptine’s use and regulation in the United States, particularly through a health equity lens that addresses racial disparities in treatment and outcomes for Black women.
Given the opioid-like effects of tianeptine, healthcare providers should be vigilant for signs of intoxication or withdrawal, which may not be detected through standard urine drug screenings.29 There is a pressing need to expand screening protocols, implement early interventions, and develop informed policies regarding tianeptine. These actions should be grounded in systemic research that considers the social, regulatory, and clinical dimensions of this emerging public health concern.
Limitations
This study has several important limitations. The use of EHR data depends on accurate documentation and coding. Because tianeptine is often sold under nonpharmaceutical names such as ZaZa, Red, or Tianaa and outside of formal medical settings, cases are likely underreported or misclassified within EHR systems. This could lead to an underestimation of actual use or misuse. The dataset also does not include toxicological confirmation of tianeptine exposure such as serum or urine assays measuring tianeptine or its metabolites, which may limit the accuracy of exposure classification. Many diagnoses may reflect healthcare provider suspicion or patient self-report rather than laboratory verification, which limits the validity of the findings. It is also not possible to determine the circumstances of use, whether for legitimate therapeutic reasons (particularly outside the United States), recreational misuse, or overdose, which makes interpretation more difficult.
The absence of recorded cases among certain demographic groups, including Black individuals in the early study period, limits the ability to draw definitive conclusions regarding temporal trends across race. This may reflect underreporting, differences in healthcare access, or variability in coding practices within the EHR dataset. Additionally, a substantial proportion of patients were recorded as having “Unknown” race or ethnicity, which may reduce the accuracy of demographic analyses and obscure true disparities. Furthermore, the TriNetX Global Collaborative Network does not equally represent all geographic regions or healthcare systems. Regional variation, along with differences in state-level policies regarding supplement sales and tianeptine regulation, may influence observed incidence patterns and limit the generalizability of these findings.
Socioeconomic information such as income, education level, or insurance status is also unavailable in the dataset. These factors could shape access to tianeptine or reasons for use but were not explored in this analysis. Similarly, missing details about dose, route of administration, and duration of use make it difficult to understand the severity or progression toward dependence. Finally, because the study is cross-sectional, it cannot track patients over time. This prevents examination of repeated use, escalation, or long-term outcomes such as treatment engagement or mortality.
Conclusions
The emergence of tianeptine as an opioid-like substance highlights shifting patterns in substance misuse that disproportionately impact Black females, particularly among young adults and the elderly. Notably, cases have newly emerged in younger populations, particularly adolescents and young adults, where incidence was previously absent. Our findings reveal a troubling rise in tianeptine-related toxic effects within historically underserved populations, underscoring the urgent need for targeted public health responses. The accessibility of tianeptine through unregulated channels, coupled with systemic healthcare barriers to treatment, exacerbates existing racial and gender disparities in healthcare. As this trend continues, healthcare providers, policymakers, and researchers must prioritize surveillance, education, and interventions to mitigate harm and prevent further escalation. Future studies should focus on understanding the social factors that contribute to tianeptine use, informing evidence-based policies, and improving outcomes.
Funding
None
Conflicts of interest
All authors declare no conflicts of interest