Introduction
Polypharmacy is a common phenomenon affecting middle-aged and aging populations at unprecedented rates. Though polypharmacy has different definitions, it is most commonly defined as the concurrent use of 5 or more clinically indicated medications, with excessive polypharmacy being defined as the use of 10 or more medications.1–7 It is thought to be prevalent in older populations due to comorbidities attributed to multiple organ systems.6 Among people living with HIV (PLWH), the prevalence of polypharmacy ranges from 23% to 39%, which is higher than in people living without HIV (PLWOH).4 Polypharmacy is also shown to increase the chances of detrimental drug-drug interactions and drug adverse effects, and can increase the likelihood of poor adherence to medication regimens.1,8 Polypharmacy has also been shown to be a risk factor for other preventable health outcomes such as cognitive decline, hospitalizations, and mortality. It can lead to poor mental health outcomes such as dementia and depression.1,3
Depression is a mood disorder affecting 280 million people worldwide and can alter the mental, physical, and emotional aspects of an individual’s life.9,10 It is a common problem in older adults, though not considered a normal component of aging.10 Scales such as the Center for Epidemiologic Studies Depression Scale (CES-D), Patient Health Questionnaire-9 (PHQ-9), and Geriatric Depression Scale (GDS) can help diagnose and classify symptoms of depression in older adults and those with HIV.11 Depression is also associated with increased risks of functional disability, dementia, mortality, cardiovascular events, and use of health services.3,5 In older adults, it can reduce quality of life and complicate preexisting chronic conditions.11 Depression is estimated to be 2 to 3 times higher among PLWH (22%-45%) than PLWOH (3%-17%).9 In patients with HIV, depression can affect treatment adherence, social engagements, and quality of life and can also impact life expectancy.12 One study additionally noted that in developing countries, depression can be associated with an increased risk of disease progression in HIV clinical stage III or IV, regardless of sociodemographic factors, psychosocial support, or health condition.13,14
Polypharmacy may be associated with depression due to increased medication burden and reduced adherence, both of which have negative health outcomes.1,3,8 A meta-analysis of 19 studies found that individuals, particularly older adults, taking multiple medications were at increased risk of experiencing depressive symptoms.3
This study uses cross-sectional data from a sub-study, titled “Understanding Healthy Aging Among Men Who Have Sex With Men” conducted in the Multicenter AIDS Cohort Study (MACS), an ongoing observational cohort study of middle-aged and aging men living with or without HIV in the United States. HIV-positive men have been shown to take a median of 13 medications, including medications for HIV, and display increased depression symptoms.4,15 In this study, non-HIV medications also were examined in order to more accurately capture the burden of medications used to manage comorbid conditions.4 There is a paucity of evidence on whether HIV status moderates the relationship between polypharmacy and depression. This study aims to investigate whether the association of polypharmacy increases the odds of depressive symptoms in PLWH vs PLWOH.
Methods
Study Population
The MACS is a prospective cohort study of the natural and treated history of HIV/AIDS among men who have sex with men in 4 US sites: Baltimore/Washington, DC; Chicago; Los Angeles; and Pittsburgh/Columbus. Since its inception in 1984, a total of 6972 HIV-positive and HIV-negative men who have sex with men have been enrolled in the study over three time periods: 4954 in 1984-1985; 668 in 1987-1991; and 1350 in 2001-2003.16–18 MACS participants attend semiannual clinic visits that involve an Audio Computer-Assisted Self-Interview (ACASI) and a standardized clinical examination where medical history data and specimens are collected. The study design of the MACS has been described elsewhere.16–18 Detailed information regarding HIV and non-HIV medication use has been collected at every visit since the beginning of the study. An overview of the MACS is available online at https://www.niaid.nih.gov/research/multicenter-aids-cohort-study-public-data-set. Institutional review boards at each site approved the protocol, and informed consent was obtained from all study participants.
This analysis included the first visit of two consecutive visits that occurred between October 2014 to September 2015, resulting in a cohort of 2236 (1215 HIV-positive/1021 HIV-negative) men. Missing data were imputed using data from the alternate visit. It is standard practice to use data from follow-up visits and not from retrospective visits. Imputation was utilized since the likelihood that polypharmacy would change between visits is low, especially for those who have polypharmacy.
Outcome
Depression
Possible risk of clinical depression was assessed using the CES-D. The CES-D is a 20-item self-report questionnaire used to screen for depression and measure the frequency of depressive symptoms in the past week. It is widely used in both general population and clinical settings and includes items related to depressed mood, guilt, sleep and appetite disturbances, and a loss of interest. Responses are rated on a 4-point scale, and a total score from 0 to 60 is calculated, with higher scores indicating more severe depressive symptoms. A score of 16 or higher was used as a cut-off point to suggest a possible risk of clinical depression, as other articles suggest.19,20
Primary Predictor
Polypharmacy
Polypharmacy was defined using a dichotomous indicator 5/<5) of five or more non-HIV medication classifications taken since the participant’s last visit. At each visit, a binary variable for medication classifications was used to classify whether the participant had used any medications in that classification since their last visit. Routinely used and as needed medications were treated similarly.
As part of routine data collection and processing during each semi-annual visit, data on self-reported non-HIV medications were collected, given a common drug code, and grouped into general drug classifications: cholesterol lowering, antihypertensive, diabetes drug, hepatitis C virus drug, hepatitis B virus drug, steroids, hormones, anticancer, antidepressants, tranquilizers, aspirin, antibiotics, and unclassified. For this analysis, additional drug classifications were created for drug codes that were originally labeled “unclassified” or did not belong to a classified group. These new classifications were antihistamine, appetite suppressant, antianginal, anticoagulants, antidiarrheal, antifungal, anti-ulcer, central nervous system stimulants, digestive/biliary, dopamine, herbal supplements, muscle relaxants, nonsteroidal anti-inflammatory drugs, opioids, substance abuse treatments, tuberculosis, and vitamins. Medications with very low prevalence were combined into an “other” medication category. There was a total of 30 medication classifications in our analysis. Non-HIV medications included prescription and nonprescription drugs and excluded recreational drug use.
Covariates
Sociodemographic Characteristics
Race/ethnicity at baseline was categorized as White non-Hispanic, Black non-Hispanic, and other. Age at each visit was calculated from the self-reported date of birth and date at visit and categorized as younger than 50 or older than or equal to 50 years. Enrollment was classified into early recruitment (1987-1991) and later recruitment (2001-current).
Comorbidities
Selected comorbidities were examined and included high blood pressure (systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg), diabetes (fasting glucose ≥126 mM), liver disease (serum glutamic pyruvic transaminase or serum glutamic oxaloacetic transaminase >150 UL), kidney disease (estimated glomerular filtration rate <60 mL/min/1.73 m2 or urine protein-to-creatinine ratio ≥200), and dyslipidemia (total cholesterol ≥200 mg/dL or low density lipid ≥130 mg/dL or high density lipid <40 mg/dL or triglyceride ≥150 mg/dL).
Insurance Coverage
Health Insurance coverage was defined using self-reported responses to the question “Are you currently insured?” Participants responded with “Yes.”
HIV-Related Risk Factors
HIV serostatus (positive/negative) was assessed using enzyme-linked immunosorbent assay with confirmatory Western blot on all MACS participants at their initial visit. If a participant tested HIV-negative at baseline, they continued to be tested at every subsequent visit to confirm they remained HIV-negative. HIV-positive participants included all men who were identified as such at baseline and those who seroconverted during study observation. CD4+ T-lymphocyte cell counts (cells/mm3, CD4) and plasma HIV RNA levels (viral load, copies/mL) were collected among participants with HIV. CD4 counts and HIV RNA viral load were dichotomized into <500 cells/mm3 and 500 cells/mm3 and detectable or undetectable (based on the lower detection level of the assay used at visit), respectively.
Statistical Analysis
Descriptive statistics were generated for the outcomes and covariates using frequencies and percentages for categorical variables and medians and interquartile ranges for continuous variables. Multivariable logistic regression models were used to estimate the association between polypharmacy and depression, adjusting for race and ethnicity, education, insurance status, and number of health care visits. The multivariable model for the overall sample included an age and HIV status combination variable, while the PLWH sample included the additional variables age, AIDS diagnosis, and viral load detected. Variables were selected from univariate analyses for candidate variables on the overall sample, while adjusting for age, race, education, and insurance. Variables with a P value less than or equal to .10 and those with importance based on the literature were included in the multivariable model. Odds ratios (ORs) and 95% confidence intervals (CIs) were reported. All analyses were performed using the statistical software R version 4.4.3, with libraries including ggplot2, gtsummary, and forestmodel.
Results
Participant Characteristics
In our sample (N=2236), 54.3% of participants (n=1215) were PLWH, and 45.7% (n=1021) were PLWOH. Among PLWH, 28% had depressive symptoms, compared with 24% of PLWOH, representing 26% overall. Polypharmacy use was listed in 42% of PLWH and 44% of PLWOH (43% overall). Overall, 74% of patients were older than 50 years (PLWH, 67%; PLWOH, 83%), with 62% identifying as non-Hispanic White and 80% having at least some college education. Most participants had insurance coverage (94%), had a median of 2 physician visits, and did not seek medical and/or dental care or prescription drugs (10%). The overall prevalence of hypertension, diabetes, and dyslipidemia were 57%, 15%, and 77%, respectively, with PLWH reporting 55%, 15%, and 79% and PLWOH reporting 59%, 14%, and 75%, respectively. Among PLWH, potent antiretroviral therapy was the dominant type of therapy used since last visit (90%), and participants had a median of 3 counts of nucleoside/nucleotide reverse transcriptase inhibitor, protease inhibitor, non-nucleoside reverse transcriptase inhibitor, enzyme inhibitor, and class II drug use. The majority of PLWH (73%) had CD4+ cells of 500 or more. Further details stratified by HIV status are given in Table 1.
Adjusted Associations of Polypharmacy and Depression
All multivariable variables were significant in the univariate analysis (P<.10) except for AIDS diagnosis, dyslipidemia, and number of comorbidities. AIDS diagnosis was included in the multivariable model due to its importance in the literature.
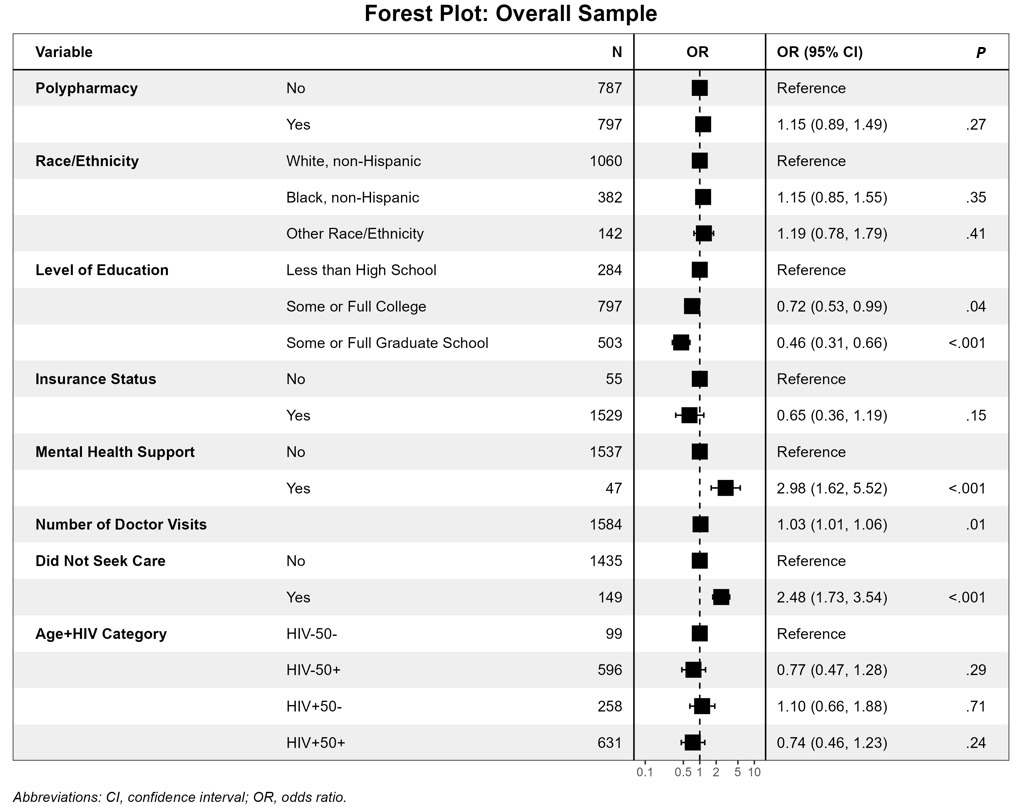
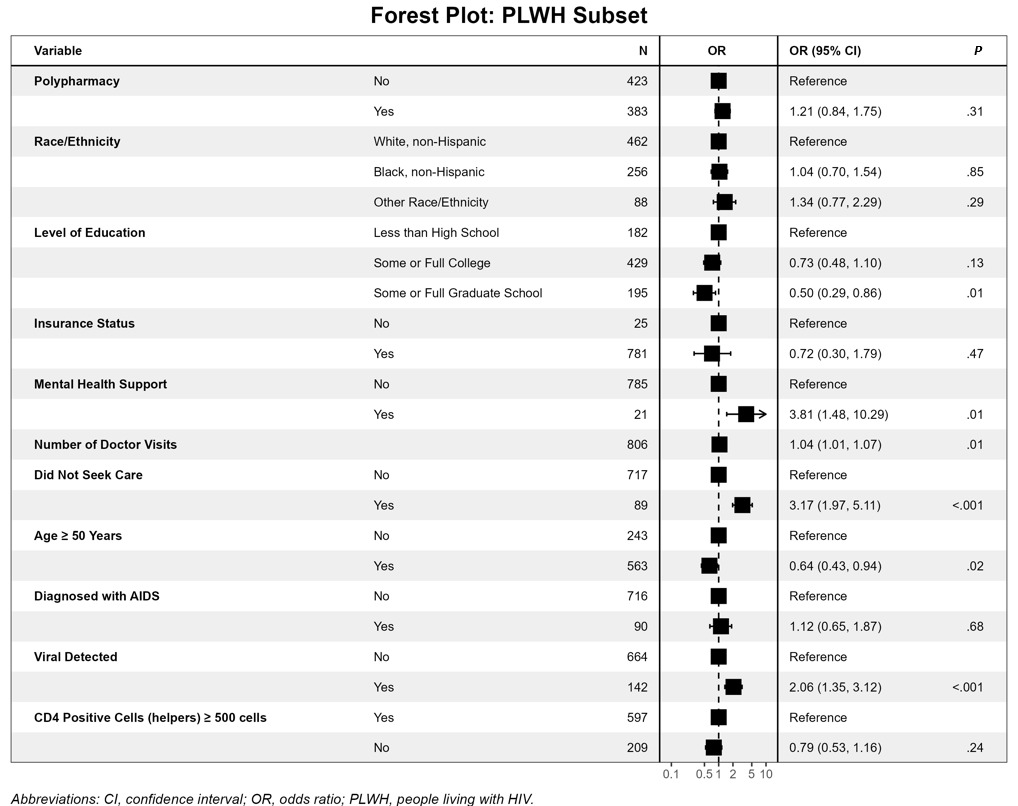
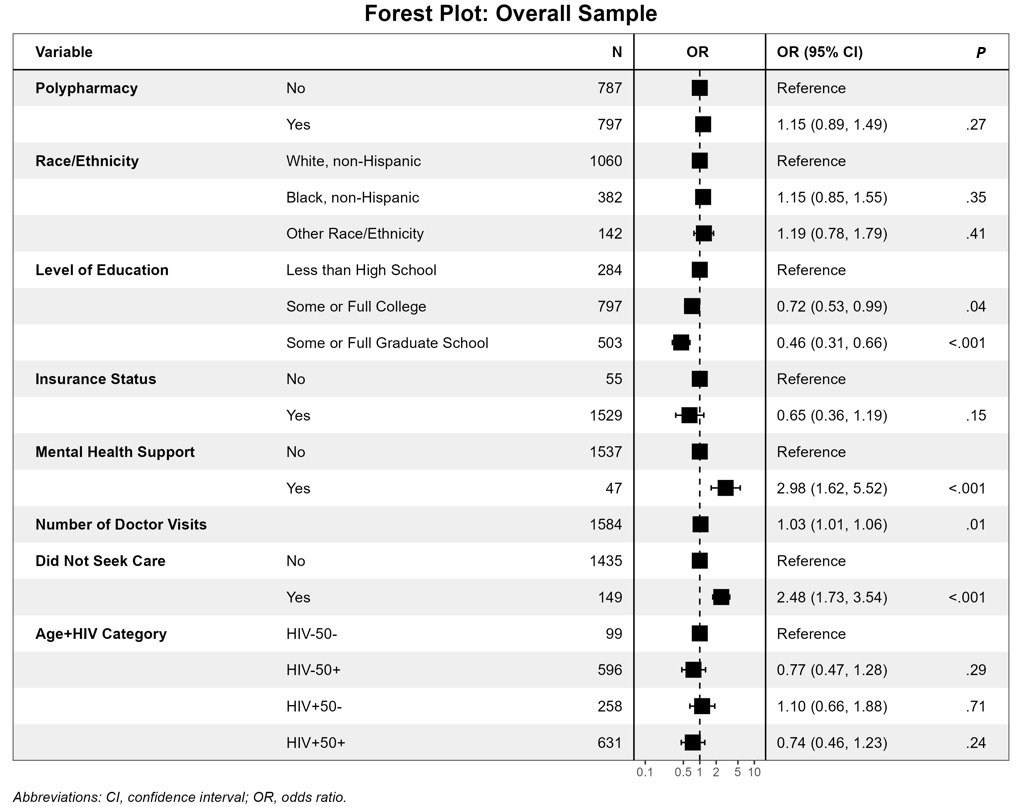
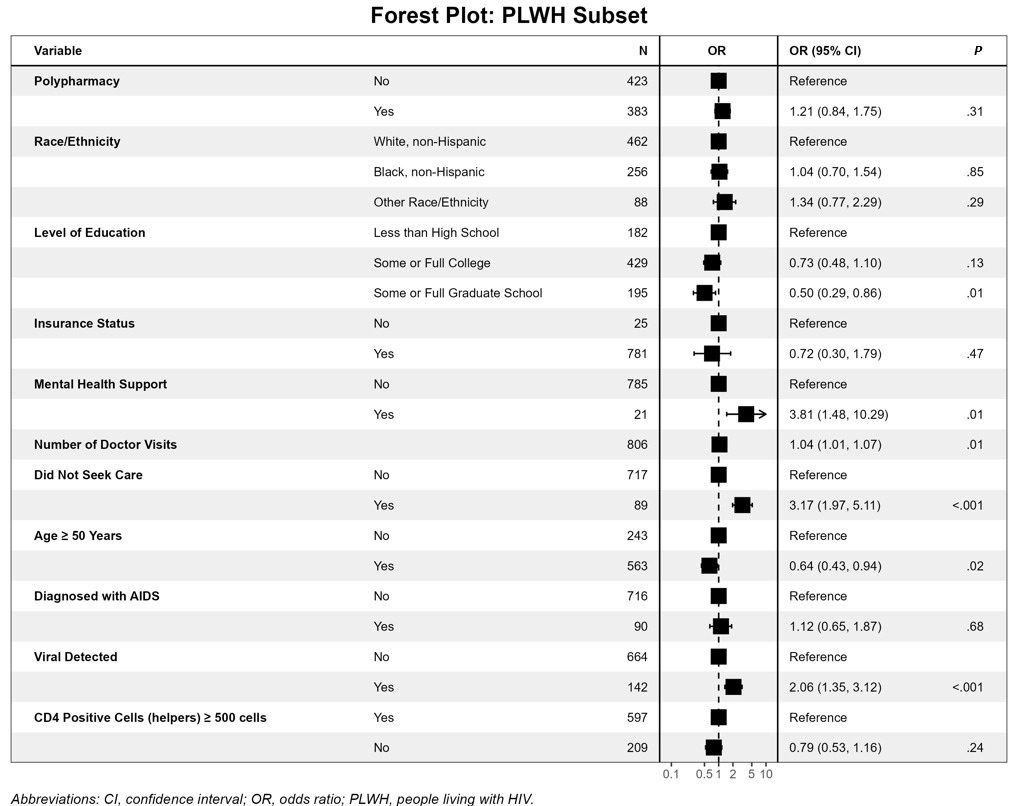
Albeit not statistically significant, polypharmacy use had a positive association with depressive symptoms (OR, 1.15; 95% CI, 0.89-1.49, P=.27) compared with those not using polypharmacy after adjusting for covariates (Table 2). In the PLWH subset, there was also a positive, not statistically significant, association (OR, 1.21; 95% CI, 0.84-1.75, P=.31).
Regarding the overall sample, covariates associated with significant decreased odds of having depressive symptoms included having some or full graduate school compared with less than high school (OR, 0.46; 95% CI, 0.31-0.66, P<.001). Covariates associated with statistically significant increased odds of having depressive symptoms were seeing a doctor concerning depression, anxiety, or mental health problem (OR, 2.98; 95% CI, 1.62-5.52, P<.001), number of doctor’s office visits (OR, 1.03; 1.01-1.06, P=.006), and did not seek medical and/or dental care or prescription drugs (OR, 2.48; 95% CI, 1.73-3.54, P<.001). Variables with non–statistically significant decreased odds of having depressive symptoms included having insurance coverage (OR, 0.65; 95% CI, 0.36-1.19, P=.15) and being HIV+ 50+ compared with being HIV- 50- (OR, 0.74; 95% CI, 0.46-1.23, P=.24); variables with increased odds included being non-Hispanic Black compared with non-Hispanic White (OR, 1.15; 95% CI, 0.85-1.55, P=.35) (Figure 1).
Among PLWH, a statistically significant increase in the odds of having depressive symptoms was associated with the variables seeing a doctor concerning depression, anxiety, or mental health problem (OR, 3.81; 95% CI, 1.48-10.29, P=.006), number of doctor’s office visits (OR, 1.04; 95% CI, 1.01-1.07, P=.01), not seeking medical and/or dental care or prescription drugs (OR, 3.17; 95% CI, 1.97-5.11, P<.001), and having viral load detected (OR, 2.06; 95% CI, 1.35-3.12, P=.001. Being non-Hispanic Black (OR, 1.04; 95% CI, 0.70-1.54, P=.86), and having an AIDS diagnosis (OR, 1.12; 95% CI, 0.65-1.87, P=.68) were non–statistically significantly associated with increased odds of having depressive symptoms. Statistically significant decreased odds of having depressive symptoms in PLWH were found in those who had some or full graduate school (OR, 0.50; 95% CI, 0.29-0.86, P=.01) and in those who were older than 50 years (OR, 0.64; 95% CI, 0.43-0.94, P=.02). Having less than 500 CD4+ cells (OR, 0.79; 95% CI, 0.53-1.16, P=.24) and having insurance coverage (OR, 0.72; 95% CI, 0.30-1.79, P=.47) were non–statistically significantly associated with decreased odds of having depressive symptoms (Figure 2).
Discussion
In this study, among men living with or without HIV, polypharmacy was associated with having depressive symptoms; however, the association was not statistically significant. This finding was similar but also not statistically significant when examining only the men living with HIV.
A systematic review and meta-analysis by Palapinyo et al3 looked at 19 studies and found evidence that individuals taking more medications were at an increased risk of experiencing depression; however, this study did not look at people who were living with HIV.
Among all the men, the variables not being non-Hispanic White and being HIV positive and younger than 50 years were positively associated with having depressive symptoms. Although these associations were not statistically significant, they warrant further investigation. Identifying as a specific ethnicity helps explain the relationship between polypharmacy and depression, as research has found that ethnic minorities are less likely to initiate antidepressant treatment than non-Hispanic White patients, leading to a higher likelihood of having depressive symptoms.18 Furthermore, other studies have found that men living with HIV who are younger than 50 years were more likely to have depressive symptoms than those who were older than 50 years, most likely due to the various challenges associated with the younger age group, such as child rearing, financial hardships, domestic problems, or lack of support.21 Being HIV positive and older than 50 years compared with being HIV negative and younger than 50 years was negatively associated with having depressive symptoms. This finding did not explain the relationship between polypharmacy and depression, as older men with HIV tend to have more comorbidities and therefore may need more medications to treat their conditions.22 However, in some cohorts, older men with HIV may have higher levels of grit and individual-level psychosocial reliance factors, which may reduce their likelihood of depression.23 Additionally, polypharmacy in PLWH has been linked to poorer health outcomes and worsened quality of life, which may contribute to having more depressive symptoms.24
Regarding men living with HIV, those who were not virally suppressed and were immunosuppressed were more likely to have depressive symptoms. Men in the highest tertile of depressive symptoms have been found to have a higher risk of having an unsuppressed viral load, explaining the positive association between depressive symptoms and poor virologic control.25
For both groups (PLWH and PLWOH), those who regularly sought healthcare had increased odds of having depressive symptoms, whereas those with higher education, with insurance coverage, and older than 50 years had decreased odds of having depressive symptoms. Higher levels of education and having insurance coverage may explain the relationship between polypharmacy and depression, as these factors are often associated with higher levels of income, which can help mitigate mental health outcomes related to financial strain.26 Visiting a doctor concerning mental health concerns could explain the relationship between polypharmacy and depression, as polypharmacy is linked with higher healthcare utilization.27 Furthermore, not seeking medical care also could explain the relationship between polypharmacy and depression, as nonadherence to medication regimens and unmet needs are associated with worse mental health and higher psychological distress.28
A few limitations were present in this study. Participants in the MACS were conveniently recruited and may not represent all men living with or without HIV in the United States. No women were included in this study which further limits the generalizability of these results. Additionally, reporting bias may have been present in this study, such as social desirability bias, where participants may have underreported symptoms of depression or number of medications. Furthermore, reporting bias could have also affected the number and categories of medications that were self-reported. The usage of classification-based definitions of polypharmacy may have also oversimplified the true burden of managing multiple medications. Also, the inclusion of antidepressants in the polypharmacy count could impact the association between polypharmacy and depressive symptoms. Lastly, this was a cross-sectional study design and we were therefore unable to examine the temporality of the relationship between polypharmacy and depression.
Conclusion
This work highlights the need for setting mental health screenings as a pillar of care, especially in primary care settings. These mental health screenings should also include specific questions pertaining to medication review. Routine screening tools could help clinicians identify patients who could benefit from fewer medications and those who are at high risk for developing depressive symptoms. Asking about medications can improve patient autonomy and emotional well-being, especially among populations navigating the dual challenges of aging and chronic HIV management. Integrating these findings into clinical practice will require collaborative efforts among primary care providers, mental health providers, and HIV specialists to create protocols for routine medication review and depression screening during follow-up visits. Such protocols could be placed in electronic medical record systems in order to gauge patient satisfaction and compliance with their medication regimen. Interdisciplinary approaches to understand the depression-polypharmacy relationship can help clinicians move toward more equitable and holistic care for individuals with or without HIV.
Acknowledgements
We are indebted to the participants of the Multicenter AIDS Cohort Study (MACS) Healthy Aging Study. We thank the staff at the 4 sites for implementation support and John Welty, Montserrat Tarrago, and Katherine McGowan for data support of this study.
Sources of Support
Multicenter AIDS Cohort Study (MACS) Healthy Aging Study, the staff at the 4 sites for implementation support and John Welty, Montserrat Tarrago, and Katherine McGowan for data support of this study.
The authors declare no conflict of interests.