Introduction
According to the International Society for Infectious Diseases (IDSA), global estimates suggest that approximately 6.5 million people acquire invasive fungal infections yearly, and over half of those infections result in mortality. One of these deadly infections is aspergillosis. Invasive aspergillosis (IA) develops in 2.1 million people annually, with a mortality rate of 85.2% with treatment, whereas chronic pulmonary aspergillosis (CPA) affects 1.84 million individuals annually with a mortality rate of 18.5% with treatment.1
Aspergillus fumigatus is a saprophytic mold, meaning it obtains nutrients by absorbing them from decaying matter, found in soil and compost. While the mold typically thrives in moist habitats to live, it spreads via inhalation of spores in dry environments that can be found in dust, hay barns, and compost sites.2 It is an opportunistic fungus of humans, plants, and animals.3–5 A study from the Netherlands found potential hotspots for A fumigatus included waste from flower bulbs, residential household waste (fruits, vegetables, garden scraps), landscaping waste (grass, leaves, shrubs, trees), wood chippings, exotic and regional fruit, and manure from horses, cattle, and poultry. The study found that three of these hotspots—flower bulb waste, landscaping waste, and wood chippings—had data reflecting consistent resistance, whereas the other sources did not show steady azole resistance in repeated experiments.6 Aspergillus fumigatus is known to cause a wide spectrum of infections, including allergic aspergillosis and acute life-threatening invasive infections.7
Some factors that contribute to the prevalence of A fumigatus as a human pathogen include its abundance in nature and virulence factors that allow for immune evasion and suppression. While humans may inhale over 100 spores of this mold daily, it generally does not cause illness in immunocompetent individuals, as the immune system removes the pathogen.8 In immunocompromised people the spores may begin to grow owing to lack of phagocytes, as phagocytes recruit other immune cells to help destroy the A fumigatus spores and fungi. These phagocytes include neutrophils, which prevent the formation of hyphae, fungal branch-like structures, and kill the mold by ingesting it. Once growth is established, A fumigatus may invade blood vessels and disseminate into other parts of the body, causing a multi-system infection.9 The World Health Organization named A fumigatus one of the most critical public health threats in April 2022, ranking the mold number one for public health importance and number three overall when considering both public health importance and current research and development initiatives.10 With its current rank on the WHO fungal priority pathogen list, the increase in triazole-resistant strains, high mortality rates, and its importance in both medicine and agriculture, the need for novel treatments to A fumigatus infections is more urgent than ever.
Clinical Presentation
Aspergillus fumigatus can cause a wide spectrum of symptoms in humans, with presentation severity depending largely on the immune status of the host. Three prevalent clinical presentations include IA, CPA, and allergic bronchopulmonary aspergillosis (ABPA).11 The most severe of the three is IA, which is often seen in the lungs, sinonasal cavity, and brain.12 Azole drug resistance has been linked to a 25% increase in mortality during clinical infection when compared to those with wildtype infections.13
Invasive Aspergillosis
Invasive aspergillosis affects those who are immunocompromised who have underlying illnesses such as cancer, autoimmune diseases, organ transplant, hematological disease, and respiratory infections.14,15 Invasive aspergillosis is one of the most devastating forms of A fumigatus infections owing to the opportunistic and rapidly progressing nature of the disease.16 The mold is breathed through spores in the air and hyphae attach to host epithelial cells in the lungs. These hyphae can promote invasion of blood vessels, allowing Aspergillus to travel systemically.17 Early diagnosis is important but proven to be quite a challenge owing to the nonspecific respiratory symptoms.8 Once infection is established, diagnostic imaging of the lungs can show halo signs, necrosis, mass or wedge infiltration, and cavitation, which may cause disease progression into CPA.11 Mortality rates for IA can be as high as 90%, especially in cases with delayed diagnosis. Evidence of geographic spread of IA cases is lacking owing to incomplete data; however, increased rates of azole-resistant cases have been reported, specifically surrounding Europe.18–21 Current treatment initiatives consist of azoles, polyenes, and echinocandins.22 In cases in which A fumigatus is resistant to antifungals, treatment recommendations are adjusted to amphotericin B lipid formulations or combination therapy; however, there is a lack of evidence supporting this approach.23 Other alternative therapies could include monoclonal antibodies (mAbs), which have the potential to not only improve diagnostic testing but also could form the basis for novel IA treatments. Monoclonal antibodies have been used to treat certain cancers, autoimmune diseases, asthma, and infectious diseases.24–28 However excessive cost of use is a strong limitation in the use of this personalized therapeutic option. Another option that has seen success in preclinical models is chimeric antigen receptor (CAR) T cells. In vitro and in vivo models demonstrated that T cells expressing the A fumigatus–specific CAR (Af-CAR) exerted a direct antifungal effect against A fumigatus hyphae. In vivo murine models of IPA showed that CD8 Af-CAR T cells reduced fungal burden in the lung.29 While there is potential success in this alternative treatment, there are few studies on use in fungal diseases.
Chronic Pulmonary Aspergillosis
Chronic pulmonary aspergillosis has two subtypes: chronic cavitary pulmonary aspergillosis (CCPA) and aspergillomas. Chronic cavitary pulmonary aspergillosis refers to the colonization of one or more aspergillomas in pre-existing cavities in the lungs. An aspergilloma is a network of Aspergillus hyphae, termed fungal ball. Chronic cavitary pulmonary aspergillosis most commonly occurs in immunocompetent individuals who have had previous lung disease. Prevalence is highest in those who have residual lung cavities due to tuberculosis but can also be seen in those with chronic obstructive pulmonary disease, lung cancer, and SARS-CoV-2. Chronic cavitary pulmonary aspergillosis is rare to see in the United States, with one case per 100,000 individuals per year. Prevalence is higher in African nations, especially in areas where tuberculosis infection rates are higher.2 Aspergilloma may completely fill the cavity they develop in, causing it to become a danger to the host and require removal.30 While a solitary aspergilloma causes the patient little to no symptoms, CCPA is associated with significant pulmonary or systemic symptoms and can progress through creating new cavities, increasing fibrosis, or increasing infiltration.2
Diagnosis of CPA is generally performed with X-ray and computed tomographic scans, which will show opacity in the pulmonary region if positive. Treatment can be difficult due to the unpredictable outcome of the aspergillomas. For example, about 10% of cases have spontaneous regression, whereas other cases progress to hemoptysis or coughing up blood. The ability to predict the severity of hemoptysis is limited. Surgical removal of a portion of the lung, known as a lobectomy, is considered the gold standard but is associated with high mortality. Current ISDA recommendation for asymptomatic CPA patients is to monitor the progression. Elevated-risk surgical candidates are given prolonged courses of triazoles. Surgical removal is still recommended for those who have symptoms and who qualify for this type of treatment.2 A recent study found that a wedge resection—a surgical alternative to a lobectomy—may be an improved surgical option, as it is associated with lower risk of complications and better early-stage outcomes. It should be noted that long-term risks have not been assessed for wedge resection, so more research will need to be performed to find the rate of recurrence, which is reported to be 5% to 26% for lobectomy cases.30 Last, antifungal therapy is a treatment option, but it is considered to have limited value in treating CPA because of resistant strains of Aspergillus. If antifungal therapy is the only viable treatment option for a patient, it is recommended to use intravenous therapies with micafungin or liposomal amphotericin B (L-AmB).31
Allergic Bronchopulmonary Aspergillosis
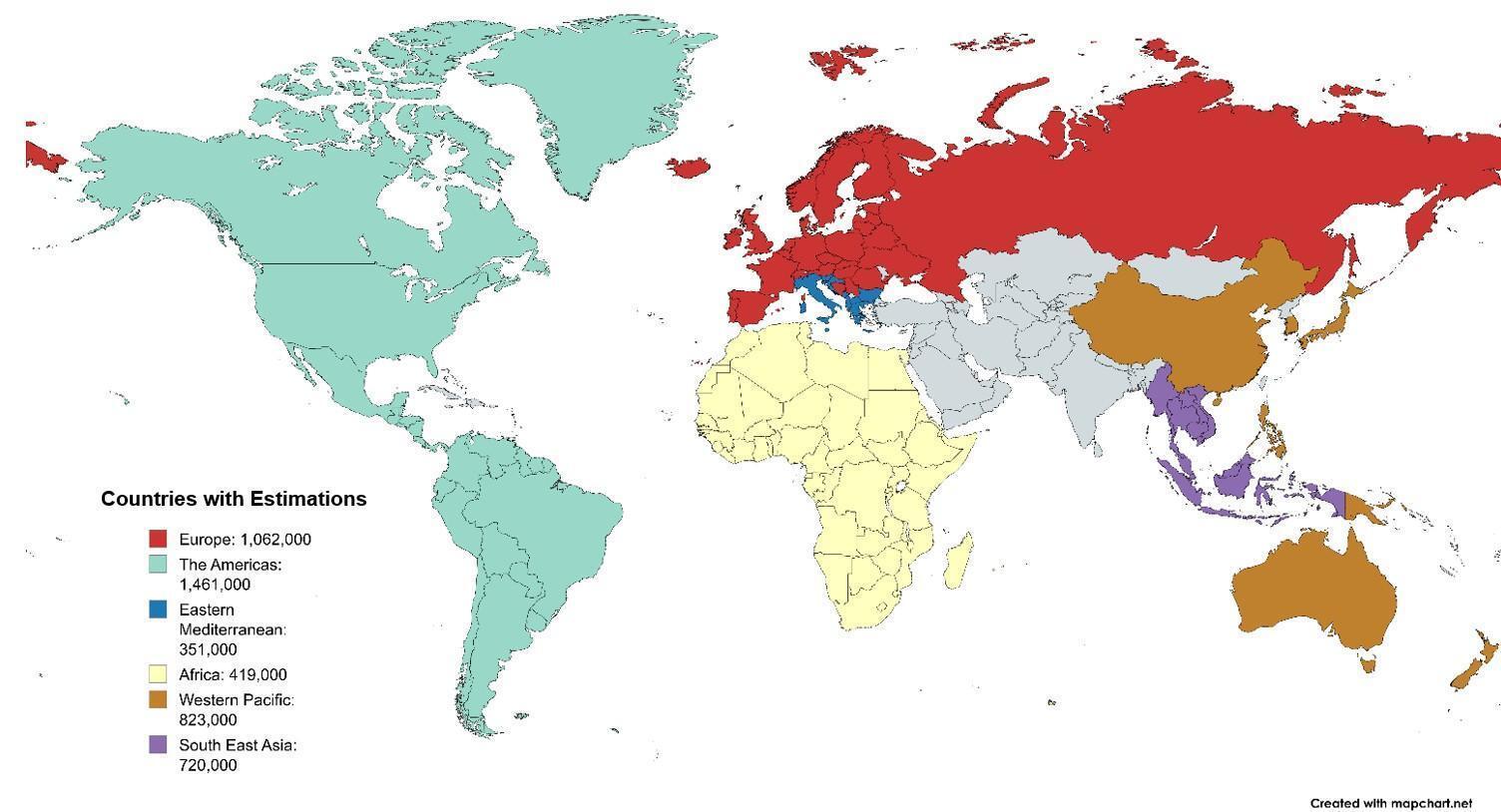
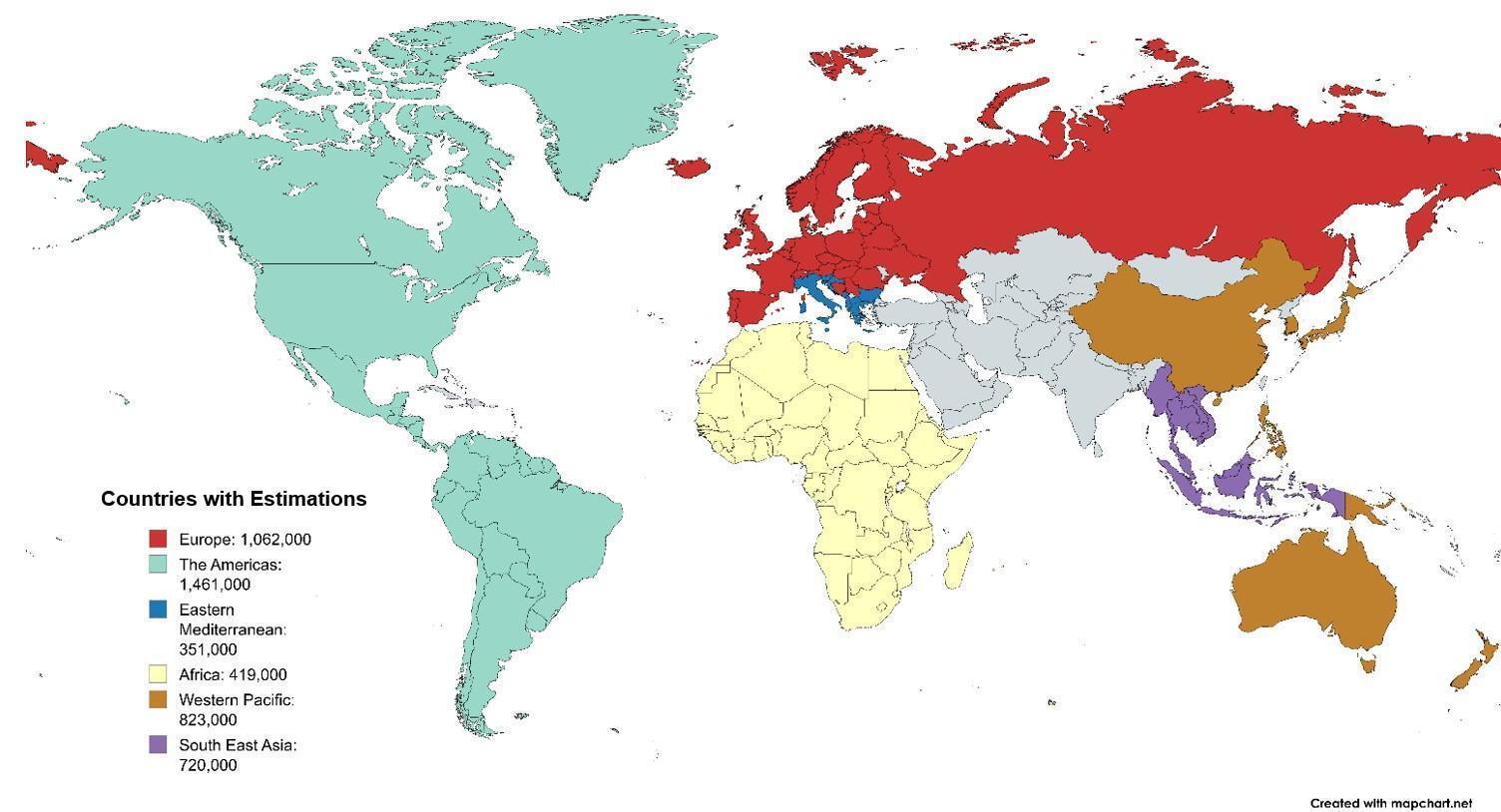
Allergic bronchopulmonary aspergillosis is a type of aspergillosis triggered by repeat exposure to A fumigatus. In 2013, the global burden of ABPA was thought to exceed 4.8 million cases per year; the distribution is shown in Figure 1.32 This clinical manifestation is commonly seen in patients who have uncontrolled asthma or cystic fibrosis, which are both conditions that affect the lungs.33
Allergic bronchopulmonary aspergillosis is often misdiagnosed as other pulmonary-associated illnesses, because it displays nonspecific symptoms such as coughing, wheezing, chest pain, and blood-stained sputum and can be seen in patients of all ages. A Japanese study found that among 75 patients, 69% were misdiagnosed.33 Due to this misdiagnosis and no clinical standard for diagnostic testing, there is often a delay in diagnosis, which can lead to complications. Current diagnostic criteria include presence of a predisposing pulmonary condition, a positive result on Aspergillus skin test, and an elevated immunoglobulin E (IgE) serum count.34 Treatment with corticosteroids remains the main drug therapy for ABPA, though these guidelines were implemented in 2000. There is a call for an update in treatment, especially because of the increase in antimicrobial resistance. An international panel developed new guidelines, including oral prednisolone or itraconazole monotherapy, for treating new cases of ABPA, and recommends a combination of these two therapies for recurrent cases.35 For cases that involve azole-resistant strains of A fumigatus in ABPA, there is limited literature on alternative treatments, but humanized mAbs have seen success, particularly dupilumab in one case, an anti-interlukin-4 receptor alpha antibody. Further research will be required to determine if this alternative is long lasting, as other mAbs such as mepolizumab have had decreased efficacy in clinical response to ABPA infections after 2 years of use.36
These clinical manifestations differ in severity, host susceptibility, and treatment approaches and are summarized in Table 1. Invasive aspergillosis, the most severe and life-threatening type, primarily affects immunocompromised individuals. Standard antifungal therapies are used, but because of the increase in azole-resistant strains, IA has become more difficult to treat. In contrast, CPA tends to occur in immunocompetent individuals who have pre-existing lung damage. While surgery is the gold standard of treatment for this type, it has a high mortality rate and risk of recurrence. Allergic bronchopulmonary aspergillosis is often misdiagnosed and becomes harder to treat as it persists, with treatment relying on corticosteroids and, depending on severity, itraconazole. There is a potential to prevent A fumigatus infection through a vaccine that utilizes the AFMP4 antigen. Aspergillus fumigatus mannoproteins (AFMP) are glycoconjugates expressed on the fungal surface and released during fungal growth. These proteins are involved in the induction of T-cell immunity.9 There have been other successful mannoprotein vaccines, including the Haemophilus influenza type B and pneumococcal vaccines.37
One Health Perspective
With human populations growing and expanding into new geographic areas to grow food, a dynamic approach to health care is needed. This is where the One Health program comes in. The World Health Organization defines One Health as an integrative conceptual model that aims to balance and optimize the health of animals, humans, and the environment; this approach provides guidance and implementation for comprehensive plans of action that aim to control the full spectrum of disease and that benefit all three aspects (i.e., animals, humans, the environment).38 A common One Health issue is antimicrobial-resistant strains, which can quickly spread through communities as well as food supplies.39 This is a concern that is becoming more urgent with A fumigatus. The increased use of triazoles—in agriculture with fungicides and pharmacology with antifungal drugs—is thought to be a driver of antifungal resistance and will require a One Health approach to find a solution.40 Starting in 2018, a One Health campaign began that monitored hotspots, through surveillance of food and garden products, where A fumigatus could be found in the United States. The surveillance included some grocery store produce such as grapes, nuts, and apples as well as garden products like compost, soil, and tulip flower bulbs. The study found that most of the compost and flower bulbs were pan-azole resistant. Current practices include composting plant waste and using that in future crop cycles, but when current chemical usage is taken into consideration, this practice poses risk for fungus to develop resistance in order to survive. This occurs as the fungicide residue accumulates in plant waste, exerting selective pressure on the fungus. The study found that A fumigatus is ubiquitous in the United States, and multi-fungicide–resistant isolates were found in agricultural settings on both the east and west coasts. It is thought that generating integrated One Health policy recommendations would facilitate policymaking at the country level. Food security and disease management are both important for public health; therefore, it is imperative to incorporate a One Health strategy to address the increasing antifungal resistance found in A fumigatus. Possible areas of focus could include more precise methods of detection, integrating a disease management approach to minimize the overall amount of fungicide in the environment, and introducing collaborative surveillance data collection among states.41
Agricultural Aspects
Aspergillus fumigatus affects all three priorities of One Health, making it a particularly devastating pathogen. A general consensus is that the rise in antifungal-resistant strains stems from the overuse of antifungal drugs in agriculture.42–44 A German study surveyed crop fields and found low overall azole resistance rates by measuring before and after fungicide application. Between 2016 and 2018, 2,875 soil samples were taken and measured. The results showed that only 1% to 3% of the isolates would be considered resistant to azoles. It should be noted that while low, there was a consistent decrease in azole susceptibility following the growing season, but the changes were temporary and had reset by the growing season the following year.45 Other studies have shown much variation in azole susceptibility, with the Netherlands reporting a low 22% susceptibility rate; Brazil, 76%; and India, China, and the United Kingdom, 95% or higher.18,46–49 This variation in resistance could be due to different agricultural practices, as Germany primarily uses triazoles and imidazoles, whereas the Netherlands uses numerous azoles including triazoles, pyrazoles, imidazoles, and oxazoles.50,51 This could contribute to different selection pressures being put on the pathogen, as azole fungicides target the ergosterol biosynthetic pathway. Azoles disrupt the growth pathway by inducing inhibition of the sterol 14-alpha-demethylase (CYP51). Polymorphisms (having many forms) in CYP51 lead to resistant pathogens.41
To better understand the prevalence of resistance in the United States, 29 agricultural sites were sampled from the eastern states and 23 from the western states. Pan-azole–resistant A fumigatus was isolated from grapes, compost, tulips, and hemp. While sampling intensity (the number of samples reported in each study) varied widely, it was determined that azole-resistant A fumigatus was widespread in the United States.52 Pan-azole resistance among Aspergillus species, including A fumigatus, was also found in Argentina and was attributed to mutations spawned from widespread use of fungicides in agriculture.53 Elevated mutation rates in combination with the high sporulation production of A fumigatus promotes the emergence of resistance to antifungals while maintaining evolutionary fitness.54
Aspergillus fumigatus, potentially extending from postharvest contamination to food processing, becomes a concern further down the line with food production, especially when susceptible consumers may be put at risk. Foods such as cereals, spices, coffee, cocoa, legumes, fruits, vegetables, and nuts have all seen instances of A fumigatus contamination. This can happen preharvest in agriculture fields or postharvest during drying or storage stages. Detection occurred through microscopic examination, DNA extraction with polymerase chain reaction testing, and next-generation sequencing. It is important to understand, however, that the detection of this mold in food does not necessarily mean there is detection of azole-resistant strains. Further research is required for a complete understanding of whether the ingestion of contaminated food contributes to human infection.55
A 2025 study56 found that clinical isolates of A fumigatus disease are nearly identical to environmental isolates. The study found that, because of the absence of widespread routine genomic monitoring and wide dispersal of the fungus, implied genomic epidemiology alone is of limited value in determining transmission routes of fungal infection.56 However, because the clinical and environmental isolates are nearly identical, it begs the question of whether agricultural fungicides induce resistance to clinical azoles. A study13 conducted in the United Kingdom and Ireland had confirmed clinical cases of drug-resistant A fumigatus that were acquired from the environment, including plant bulbs and soil samples from a range of habitat types. Researchers utilized genomic sequencing of 218 clinical and environmental samples. They found that 49% of samples showed resistance to at least one of the antifungals tested, and 52% of samples exceeded minimum inhibitory concentration (MIC) breakpoints to itraconazole, 31% to voriconazole, and 52% to posaconazole.13 The European Committee on Antimicrobial Susceptibility Testing (EUCAST) sets current clinical breakpoints, so once a MIC numerical value is determined, it is compared with the set clinical breakpoints and is interpreted as susceptible, intermediate, or resistant to the antibiotics it was tested against.57 Principal component analysis, used for pattern recognition and exploratory data analysis, showed a lack of genetic differentiation among clinical and environmental isolates, which confirmed that humans can become infected with A fumigatus strains that originally developed resistance from fungicides used in the environment. The study also found strong genetic structures with azole-resistant alleles that showed signatures of selection at multiple loci, some of which have been identified as able to adapt in response to selection by fungicides.13
Another case showed that pan-azole–resistant A fumigatus isolates from agricultural settings in the United States and India carry mutations to fungicides from benzimidazole (MBC) and quinone outside inhibitor (QoI) classes. In addition, isolates from patients in clinical settings also carry the same alleles, conferring resistance to agricultural fungicides. The finding that 86% of the isolates from different countries carried alleles for resistance to MBC and QoI confirmed that the isolates came from an agricultural environment, providing evidence for an agricultural origin of some clinical pan-azole–resistant isolates to other fungicides.58
Propositions have been made to decrease the use of triazoles in agricultural practices, but this could lead to drastic decreases in crop yield and mean critical losses to farmers, along with threatening the global food production capacity.4 Disease-causing fungi results in approximately 20% crop loss preharvest and an additional 10% loss postharvest.59 A balance needs to be found between a more judicious use of triazoles in agriculture and preventing the diminishment of crop production and farming livelihoods. Examples of this include reduced fungicide application rate, setting limitations on the maximum number of applications per year, or limiting fungicide use to disease control and not for promoting plant growth.41 One study suggested that while fungicide use is integral to modern agriculture, a significant number of azoles are expected to disappear owing to stricter regulations, but there is no timeline as to when this reduction will happen.60
Virulence
Virulence factors are tools used by the pathogen that help it successfully invade and establish infection in a host. Luckily, these can be used against the pathogen by disrupting or neutralizing it without outright killing it. This method is beneficial, as it can lead to less selective pressure for resistance compared with traditional antibiotics.61 Aspergillus fumigatus uses several virulence mechanisms to help it invade a host, including using sirtuin E (sirE) deacetylase for full virulence, surface proteins for evasion, and urease to survive in macrophages; hijacking host immune responses to redirect phagosomes; conducting modulation of human eosinophils; and creating biofilms, which can lead to increased antifungal resistance.62–66
Sirtuin E Deacetylase
It is well established that sirtuins, a family of NAD±dependent proteins, regulate fungal growth, metabolism, stress resistance, DNA repair, and sporulation and have a hand in virulence for some Aspergillus species.67–69 A recent study found that A fumigatus has 6 sirtuin genes that are not essential to the mold’s viability but are essential for full virulence in a nonvertebrate model. Both SIRTKO (sirtuin knockout gene) and the sirE gene displayed defects in growth and cell wall stress and were avirulent in murine models. The loss of the sirE gene was seen to increase susceptibility to antifungals like voriconazole, which target the cell wall.62 This susceptibility is a mechanism that should be further explored as an alternative treatment for Aspergillus infections.
Surface Proteins for Evasion
It is important to understand how A fumigatus can evade the immune system once it enters the host, especially among those who are immunocompromised. Understanding these virulent mechanisms may influence procedure in a clinical setting and aid in early diagnosis, which has proven difficult, as noted above. A 2024 study63 set out to fill in these gaps of knowledge and found that A fumigatus produces surface proteins that are important for maintaining attachment structures or preventing immune recognition. Several of the proteins affect interaction with host cells through modulating survival in host cells, invasion and damage to epithelial cells, and production of cytokines. It was found that a gene known as AspA was important in modulating the inflammatory response and may be involved in the escape of phagosomal killing.63
Urease-Mediated Survival
Another mechanism of immune evasion is the use of urease to prevent phagosome acidification after macrophage uptake. Urease is hydrolyzed into ammonia and carbamate. The ammonia increases the pH of the phagosome, which neutralizes its otherwise acidic environment, preventing activation of lysosome hydrolases, thus preventing phagolysosome maturation and promoting spore survival. One study found that ureB, a structural urease, as well as maturation ureases ureD, ureF, and ureG, are necessary for enzyme activation. Without the presence of these ureases, A fumigatus is unable to use urea as a nitrogen source. Functional studies showed that urease allows the conidia—asexual nonmotile spores—to prevent phagosome acidification inside macrophages, which in turn increases survival. Additionally, the same study found that exploiting the enzyme’s dependence on nickel promoted conidial killing by macrophages and improved survival in murine models. Nickel is critical for A fumigatus urease system activity but is not a needed element for humans. This finding establishes another promising alternative to treatment with triazoles by using the nickel-chelator dimethylglyoxime.64
Phagosome Redirection
Once fungal pathogens enter the body, the immune system will typically traffic the internalized conidia into degradative phagolysosomes for clearance. Aspergillus fumigatus has found a way around this by using the fungal surface protein HscA to bind to the human protein p11 on the phagosomal membrane. This action leads to the redirection of conidia-containing phagosomes into a nondegradative recycling pathway. The interaction between p11 and HscA creates a permissive niche for fungal survival. In one study,65 a single nucleotide polymorphism (SNP) was found in the p11 gene that reduced p11 susceptibility, which resulted in better clearance of conidia and reduced IPA risk.
Modulation of Eosinophils
Some virulence factors aid in disease-specific instances. For example, A fumigatus is able to take control of host eosinophils, a type of white blood cell that plays a role in the immune response during allergic reactions, such as ABPA.66 A previous study showed nucleotide-binding oligomerization domain-containing protein 2 (NOD2) activated human eosinophils during infection, which suggested that cellular responses are important for eosinophil modulation at inflamed locations.70 A 2025 study66 supported these findings and explained how A fumigatus was able to take advantage of this mechanism. The study found that eosinophil modulation by Aspergillus extract is mediated through NOD2. Applying NOD2 inhibitors may provide a new therapeutic avenue for fungus-associated allergic diseases. The study also found that upregulation of oxidative stress-related molecules was specific to treatment with A fumigatus extract. This finding suggests that oxidative stress-related molecules can be predictors of fungal-associated allergic responses and, therefore, could be a potential therapeutic target. Modulation via NOD2 and oxidative stress may affect several functions, including adhesion, chemokine production, and release of oxidative stress proteins. It should be noted that this study used eosinophils from healthy individuals for extract stimulation; therefore, the response to fungal extracts in eosinophils from ABPA patients remains undetermined.66
Biofilm Formation
The last virulence factor to be discussed, which is also a clinical presentation of A fumigatus, is biofilms. Biofilms are an important virulent factor that contribute to antifungal resistance, making them complex to treat. They contribute to chronic and persistent infections by protecting the fungus from treatment attempts. Biofilms in Aspergillus species were first found in 2007 when scientists discovered a colony of tightly associated hyphae. The colony revealed the presence of an extracellular matrix (ECM) that acted cohesively, provided structural integrity, and was more resistant to polyenes.71
The initiation of biofilms occurs within the first 12 hours after conidial inoculation. Unlike bacterial biofilms, initiation of fungal films is driven by conidia attaching to cell surfaces and growing hyphae. The formation of immature biofilms is characterized by hyphae networks, early ECM production, and reduced antifungal susceptibility. Antifungal susceptibility is associated with efflux pump regulation, cell wall remodeling, and ergosterol biosynthesis. Mature biofilms form after roughly 24 hours and display much more complex structures as well as an abundant ECM. The antifungal resistance seen in mature biofilms is much stronger with voriconazole MIC90 greater than 256 mg/L. MIC90 is the minimum concentration of the antimicrobial needed to inhibit 90% of visible growth. The current EUCAST standards for voriconazole are VOR (>2 mg/L), which means that a result of 256 mg/L is considered highly resistant, increasing the complexity of treatment. Most infections are not diagnosed until the biofilm has become more mature, which delays treatment and increases the risk of it being unsuccessful. There is still much to learn about the Aspergillus biofilms and their potential in prophylactic treatments for susceptible populations.72 A 2025 comparison of A fumigatus and Candida albicans biofilms showed they had similar mechanisms of resistance with the ECM, efflux pumps, quorum sensing, and stress response pathways. Both pathogens adapt to host environments through epigenetic regulation and genetic mutations. Candida albicans was studied more broadly, whereas A fumigatus was studied more often in vitro. Following A fumigatus in a clinical setting could help to gain more insight into the underlying mechanisms of its biofilms and how it is able to enhance antifungal resistance.73
Conclusion
Aspergillus fumigatus remains one of the most formidable fungal pathogens due to its environmental ubiquity, adaptive capacity, and ability to cause a wide spectrum of disease, ranging from allergic syndromes to invasive, life-threatening infections. The WHO designation as a critical fungal priority pathogen underscores the urgent need for improved diagnostic tools, treatment strategies, and preventive measures. While current antifungal therapies, azoles in particular, have provided significant clinical benefit, the rising prevalence of azole resistance fueled by both medical and agricultural use highlights the limitations of relying on existing drug classes. With mortality rates for invasive disease remaining unacceptably high, particularly in immunocompromised populations, novel approaches to treatment and prevention are imperative.
From a One Health perspective, coordinated surveillance and regulation of azole use in agriculture remain vital to curbing environmental drivers of resistance. Genomic monitoring, environmental interventions, and international policy frameworks will be essential to bridge the gap between clinical and environmental health. This could include reduced fungicide application rate, setting limitations on the maximum number of applications per year, limiting fungicide use to disease control but not plant growth promotion, or creating an international database for reporting cases of resistance, which may include what antifungals the isolate is resistant against, how resistant the isolate is, and where the isolate was found. A global database may allow for a more collaborative effort in the fight against antifungal-resistant A fumigatus strains.
Looking forward, future alternatives to traditional antifungals may emerge from several promising directions. Immunotherapeutic strategies such as mABs and CAR T-cell therapies have already demonstrated efficacy in preclinical models, offering the potential to harness host immunity against fungal targets. Similarly, vaccines based on fungal mannoproteins, such as AFMP4, could serve as preventive measures for high-risk populations, following the successful model of glycoconjugate vaccines in bacterial infections. Anti-virulence approaches represent another attractive avenue; rather than targeting fungal viability, these strategies disrupt pathogenic mechanisms, including biofilm formation, immune evasion, and metabolic enzymes such as sirtuins and ureases, potentially reducing selective pressure for resistance. Moreover, host-directed therapies aimed at modulating immune responses, such as targeting NOD2-mediated eosinophil activation in ABPA or exploiting genetic resistance mechanisms, may provide individualized avenues of intervention.
The fight against A. fumigatus will require a multifaceted approach that integrates antifungal stewardship, innovative immunotherapies, and global One Health initiatives. By combining these strategies, the field can move toward more effective, sustainable, and equitable solutions that address both treatment and prevention of Aspergillus-related disease.
Correspondence
Department of Microbiology and Immunology, Georgetown University School of Medicine, 3900 Reservoir Rd NW, Washington, DC 20007
Author Contributions
Samantha Peltak: Conceptualization, Investigation, Original Draft Preparation, Visualization; Tomoko Steen: Supervision, Funding Acquisition, Review, Editing
Conflict of Interest
None reported.