Introduction
Although melanomas of the uvea are considered rare, they are the most common primary tumor of the eye in adults. The uvea is the middle layer of the wall of the eye, and is comprised of the ciliary body, iris, and choroid, with the choroid being the most common location of uveal melanoma (90% of cases).1 A melanoma is a malignant proliferation of melanocytes, and is the deadliest form of skin cancer, leading to 59,800 deaths globally in 2015.2 Between 1973 to 2013, there were 4999 cases of uveal melanoma in the United States, which is an incidence of 5.2 per million per year.3 Worldwide, there is an estimated 7095 cases of uveal melanoma annually.4 Most patients present with uveal melanoma between the ages of 50 and 70, and rarely present prior to adulthood. There are multiple identified risk factors, including fair skin, light colored eyes, congenital ocular melanocytosis, melanocytoma and the BAP1-tumor predisposition syndrome.5 These patients may present with blurred or distorted vision, visual field loss or photopsia, but they are commonly asymptomatic as well and may be identified during routine exams. Newer treatments aim to conserve the eye and may incorporate radiotherapy, phototherapy, and local excision. Regardless of treatment, nearly 50% of uveal melanoma may metastasize, usually via hematogenous spread.6 The purpose of this review is to explore the risk factors, presentation, diagnosis, prognosis, and management of uveal melanoma.
Risk Factors
Uveal melanoma, like other melanomas, most commonly arise in the Caucasian population. This is likely secondary to the protective effect of ocular pigmentation in populations from lower latitudes from UV-light induced DNA damage to melanocytes. Meta-analyses have shown both fair skin (OR, 1.8) and light iris color (OR, 1.7) to be significantly associated with the development of uveal melanoma.7 Other known risk factors for melanomas, such as increasing age, male gender, and sunlight exposure, are also associated with an increased risk of uveal melanoma.8 A case control study showed a positive association between total time outdoors (OR, 1.6) as well as occupation as a farmer (OR, 1.5), and development of choroid and ciliary body melanoma.9 Surprisingly, there is not enough evidence to suggest that occupational UV light exposure is an independent risk factor for development of uveal melanoma, although blue-light exposure (associated with arc-welding) has been shown to increase progression of uveal melanoma.10 In addition, the presence of both cutaneous and ocular nevi is also associated with this disease with relative risks of 4.36 and 4.22, respectively.11 A somatic or germline mutation of BAP1, a recently discovered tumor suppressor gene, is also associated with the development of uveal melanoma, with 5% of blood samples from patients with uveal melanoma showing BAP1 polymorphisms.12 BAP1 serves as a tumor suppressor via its deubiquitinase activity that regulates target genes in cell cycle control, cellular differentiation, and DNA damage repair.13 Recently, it has been discovered that the deubiquitination of type 3 inositol-1,4,5-trisphosphate receptor (IP3R3) in the endoplasmic reticulum promotes apoptosis by modulating calcium release into the cytosol and mitochondria.14 BAP1 has also been associated with other malignancies such as mesothelioma, cutaneous melanoma, and renal cell carcinoma, but the structural complex of BAP1 has not yet been completely characterized, so the impact of various polymorphisms is still not fully understood.15 Another risk factor for development of uveal melanoma is presence of a complete or partial monosomy 3, the chromosome that encompasses the BAP1 tumor suppressor gene.16 The condition that most strongly predisposes to uveal melanoma is ocular melanocytosis. Ocular melanocytosis is a benign entrapment of melanocytes in the upper third of dermis of the conjunctiva, sclera, and ipsilateral face leading to gray-blue hyperpigmentation.17 The exact relationship between these two conditions is unclear, yet 1 in 400 Caucasian patients with ocular melanocytosis will go on to develop uveal melanoma, and those with uveal melanoma are 35 times more likely to have pre-existing ocular melanocytosis.18 In addition, those with both ocular melanocytosis and uveal melanoma are twice as likely to have metastatic disease after 10 years (48% vs. 24%) from their uveal melanoma compared to those without ocular melanocytosis.19
Diagnosis
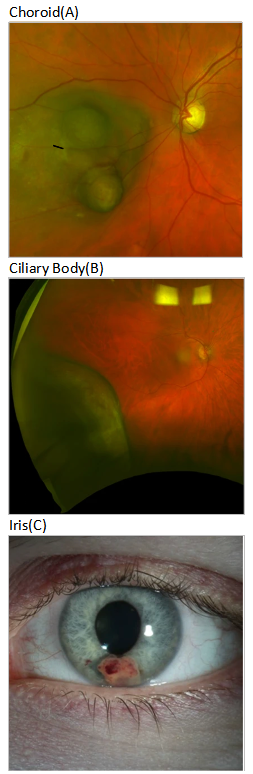
About half of all uveal melanoma will often be found on a routine eye exam in an asymptomatic patient. The other half will present with visual symptoms (flashes, floaters, visual field defects). The diagnosis of a uveal melanoma will usually begin with a slit lamp examination for iris melanomas, or with indirect ophthalmoscopy for choroidal melanomas. Aside from the pigment itself that would be appreciated grossly, the presence of orange pigment and subretinal fluid favors a diagnosis of uveal melanoma, whereas drusen and intraretinal cystic spaces are signs of a long-standing stable lesion like a benign nevus.20 Gonioscopy may also be used to assess involvement of the anterior chamber angle.
__ciliary_body(b)__and_iris_melanoma(c).png)
Subsequently, further imaging is based on the size of the tumor. For small tumors (<3mm), Anterior segment ocular coherence tomography (AS-OCT) has historically been used due to its ability to provide high resolution to anterior and lateral surfaces of the tumor. Recent studies have suggested that ultrasound biomicroscopy (UBM) is equivalent to AS-OCT for tumors in the anterior margin.22 However, for the posterior margin, UBM is superior to AS-OCT in diagnosis in that UBM is better for visualizing the tumor margin, has less tumor shadowing, and better image quality.22
Generally, noninvasive imaging (ultrasound, OCT) is sufficient for diagnosis. However, roughly 5% of cases require a biopsy since imaging may also have an overlap of findings and can be biased by subjective interpretation.23 Histopathologically, uveal melanoma can be identified and classified based on their cellular composition. The histopathological subtypes that can be identified include spindle A, spindle B, fascicular, mixed, epithelioid, and necrotic.24 Immunohistochemistry should generally reveal positivity for markers HMB45, tyrosinase, Melan-A, Sox10, and MITF. S100, generally known to be positive in melanoma, can be variable in uveal melanoma and thus is a less reliable marker.25 Nevertheless, fine-needle biopsy is now performed in most patients anyway for molecular testing to determine prognosis, as tumors with complete monosomy 3 show worse prognosis than those with partial monosomy 3 due to a larger cumulative probability of metastasis (24% vs 5.3% respectively).26
A growing number of studies have analyzed the use of blood biomarkers for not only diagnosis, but also prognosis and monitoring of uveal melanoma. These include circulating tumor cells (CTCs), circulating tumor DNA (ctDNA), and circulating MicroRNA (cmiRNA). CTCs can be extracted from blood, isolated using immunomagnetic beads, and quantified using RT-PCR.21 Studies using gp100 and CD63 for isolation of CTCs have achieved as much as a 94% detection rate for uveal melanoma.27 In addition, CTCs are not found in patients with ocular nevi.28 Thus CTCs seem to be both sensitive and specific for a minimally invasive diagnosis of uveal melanoma, but given the limited research, more validation is required. CtDNA and cmiRNA can also be extracted from blood and detected by PCR.21 Perhaps the most sensitive marker, CtDNA was detected in the blood of 100% of patients with uveal melanoma, but also detected in 50% of patients with ocular nevi.29 CmiRNA was used to differentiate benign uveal nevi from uveal melanoma with 93% sensitivity and 100% specificity.30 However, the studies examining the diagnostic value of ctDNA and cmiRNA have been limited and the number of participants have been low, so further validation is required in order for these to become relevant.
Differential Diagnosis
The differential diagnosis for uveal melanoma can be broad. All types of uveal melanoma can be mistaken for nevi, since there can be a size overlap between large nevi and small uveal melanoma.31 Statistically, between thicknesses of 2.5-3mm, there will be 5 nevi for every melanoma.31 In addition, uveal melanoma can also be mistaken for metastasis, particularly from primary lung and breast carcinoma.32 Like uveal melanoma, a metastasis may also present as a solitary yellow mass with associated subretinal fluid, and an ultrasound confirmed echodensity. 67% of primary cancer was detected prior to detection of the uveal tumor.32 As with primary uveal melanoma, metastatic lesions to the uvea may also be asymptomatic, or may present with visual impairment with or without metamorphopsia due to involvement of the macula. The choroid is the predominant location of metastasis to the uvea, making up 81% of metastatic lesions.33 This is likely because metastasis to the uvea is typically bloodborne, and the choroid is supplied by the large posterior ciliary artery with extensive anastomotic communication between choroidal vessels.34 If a possibly malignant uveal lesion is identified, it would be necessary to also conduct age-appropriate cancer screening to rule out the presence of metastasis.
Iris melanoma also has a distinct differential, which can include ocular melanocytosis, leiomyoma, iris cysts, sarcoidosis, and juvenile xanthogranuloma.35 Melanoma of the ciliary body and choroid are often differentially diagnosed with peripheral exudative hemorrhagic chorioretinopathy, congenital hypertrophy of the retinal pigment epithelium, circumscribed choroidal hemangioma, and age-related macular degeneration.36 Table 1 and 2 outline the imaging and histologic distinctions between these other lesions and uveal melanoma.
Prognosis
Local treatment of primary uveal melanoma has been shown to be effective at preventing local recurrence in 95% of cases. However, half of diagnosed uveal melanoma are at risk of metastasis likely due to the tumor’s predilection towards early micrometastasis followed by a latency period prior to the onset of overt metastatic disease.51 Features that influence the prognosis of uveal melanoma can be divided into clinical, histopathologic, cytogenetic, and gene expression features.
Clinically, factors that contribute to a worse prognosis include increasing patient age, size of tumor, ciliary body involvement, and extrascleral tumor extension.52 The American Joint Committee on Cancer Classification (AJCC) uses clinical factors based on TNM grading to create a prognostic stage from I through IV.53 T is organized based on basal diameter and thickness as well as ciliary body involvement and extraocular extension. N is based on lymph node involvement, and M is based on distance and size of metastasis. The risk of metastasis and death increased approximately three-fold for each tumor stage.54
In terms of chromosomal markers, monosomy 3 and gain of chromosome 8q have been shown to have a higher frequency of metastasis than tumors without these mutations.55 Although partial losses of chromosome 3 encompassing the BAP1 locus are associated with lower metastasis-free survival in uveal melanoma, patients with BAP1-positive monosomy 3 have prolonged survival than patients with BAP1- negative monosomy 3.56 Perhaps the prognosis of patients with monosomy 3 is truly secondary to the loss of the BAP-1 tumor suppressor gene, but more research is necessary to substantiate this claim. In addition to its possible future diagnostic significance, one study found cmiRNA that are specifically associated with monosomy 3 can be detected in blood,57 perhaps providing a route for prognostication without having to biopsy the eye.
Another highly valued prognostic indicator is a 15 gene expression profiling (GEP) assay known as DecisionDx-UM, which groups tumors into low (class 1) or high (class 2) metastatic potential based on the presence of 12 discriminating genes and 3 control genes.58 DecisionDX-UM successfully confirmed uveal melanoma in 97% of fine-needle biopsy cases in a large, prospective multicenter study.59 The 12 discriminating genes are shown in Table 3 with the associated direction of change for class 2 tumors. Note that the three control genes MRPS21, RBM23, and SAP130, are expressed in similar levels in class 1 and class 2 tumors.60
Oftentimes, clinical staging and molecular prognostication can be discordant. To balance the prognostic value of these modalities, it may be possible to combine the results of each to create a composite score reflecting a more precise prognosis. Recent studies have attempted to combine AJCC staging and GEP and have created a total risk score that seems to provide an accurate prognosis for uveal melanoma.61 Another study combined AJCC staging with chromosome 3 and 8q status and found this to provide more of an accurate prognostication of uveal melanoma. This study found that a normal genetic status of chromosomes 3 and 8 minimized the prognostic effect of AJCC staging.62 Nonetheless, more research is needed to substantiate staging using composites from these modalities. Above all, timely detection of uveal melanoma is necessary to improve prognosis.
Management
The route physicians decide in treating a uveal melanoma is highly variable and is often based on the size, symptoms, molecular markers, and metastasis. For small, asymptomatic tumors (<12 mm), it may be suitable to observe. For lesions of the choroid that are either nevi or indeterminate, research suggests these have very low malignant potential and therefore are often observed as well.59 Modalities for monitoring can vary from ocular coherence tomography, ultrasonography, or fundus photography, with follow-ups ranging between 2-4 months.
The most common method for treatment for primary uveal melanoma is radiation therapy. Namely, plaque brachytherapy is mostly used for uveal melanoma <18 mm in diameter and <12 mm in thickness. Plaque brachytherapy involves placing radioactive seeds within the eye near the tumor and using a gold sheet to protect the body from the radiation. Iodine-125 as a radiation source is the most preferred due to its accessibility in the United States, as well as it’s utility across a broad range of tumor sizes.63 Research shows no significant difference in survival rate for medium-sized choroidal melanoma treated with plaque brachytherapy compared to the previous gold-standard: enucleation.64 Enucleation is the removal of the eye itself, while leaving behind the eyelids and muscles of the eye.
Another less commonly sought out radiation option for treatment of uveal melanoma is charged-particle radiation therapy (CPRT). Charged particles can include protons, carbon ions, and helium ions. The technique localizes a high-dose region around the tumor volume and allows critical structures 3-4 mm away from the edge of the tumor to be spared from radiation.65 Although local control rates between plaque brachytherapy and CPRT are similar,66 more anterior segment complications such as eyelash loss, dry eyes, and neovascular glaucoma, arose from the helium-ion irradiation applied by CPRT.67 Though, CPRT may be appropriate for patients with disease encircling the optic nerve as it is not possible to place brachytherapy plaques around the tumor.68 Compared to brachytherapy, CPRT is more radiation-sparing to other structures outside the region of radiation. Thus, CPRT is also preferred with large tumors in patients who cannot afford to sacrifice eyesight in the ipsilateral eye, such as people who had previously lost eyesight in the contralateral eye.69
Another therapeutic option for patients with uveal melanoma is surgery. Local resection is seldom used without adjuvant therapy because of the likelihood of post-operative complications such as vitreous hemorrhage, rhegmatogenous retinal detachment, and proliferative vitreoretinopathy.70 For physicians that continue to perform local resection, adjuvant proton beam radiotherapy prior, or plaque brachytherapy after is often implemented.71,72 The previous gold-standard for treatment of uveal melanoma was enucleation. As stated prior, plaque brachytherapy is currently preferred over enucleation since studies show no additional survival benefit with enucleation.64 However, patients with uveal melanoma >18 mm in diameter and >12 mm in thickness, with moderate extraocular extension and poor visual potential are advised to receive enucleation rather than brachytherapy.73 With patients that elect for enucleation, there has been shown to be no benefit to pre-treatment with radiation therapy to the eye and orbit.74 Orbital exenteration, which is the removal of the eye, eyelids, and eye muscles, may be preferred for those with large areas of extraocular extension.
Other less invasive techniques include thermotherapy, including transpupillary thermotherapy (TTT) and photodynamic thermotherapy (PDT). TTT involves using a diode 810 nm laser light through a dilated pupil to the tumor surface. Gradually, the tumor heats up to 45-60o Celsius, which in theory obliterates tumor blood vessels leading to tumor necrosis.75 However, TTT has a maximum penetration of 4 mm,75 thus is only used for primary treatment of uveal melanoma <3 mm in thickness.76 Also, the effect of TTT on vasculature is associated with complications including retinal artery occlusion, macular edema, vitreous hemorrhage, and epiretinal membrane.76 PDT, a procedure commonly used for wet macular degeneration, is when a photosensitizer like Verteporfin is injected directly into the tumor tissue and then activated with light at a specific wavelength. This not only destroys the tumor via direct cytotoxicity, but also obliterates tumor vasculature and stimulates autophagy via a localized inflammatory reaction.77 Although PDT is not generally used as a primary treatment for uveal melanoma, it does show efficacy in small, pigmented posterior pole choroidal melanomas, achieving short-term tumor control in 80% of patients.78
In recent years, new technologies have been proposed for the treatment of many solid tumors, including uveal melanoma. These options include High-intensity focused ultrasound (HIFU), iontophoresis and electrochemotherapy (ECT). HIFU can be used to quickly heat up a local area to temperatures above 56 C, leading to coagulation necrosis without affecting the tissue vascular system.79 HIFU has been clinically used to treat malignancies such as hepatocellular carcinoma and prostate cancer.80,81 However, to treat malignancies of the eye, HIFU beams would need to function at a frequency of >10 MHz.82 Such devices have yet to be created. Iontophoresis is a technique using a low-intensity electric current to increase the biodistribution of ionized drugs, including antimetabolites like bleomycin and carboplatin.79 One study showed a dose-dependent inhibition of neuroblastoma in mice using iontophoresis of carboplatin, without any corneal toxicity at doses under 10mg/mL.83 Levels of carboplatin in the retina, choroid, vitreous humor, and optic nerve were higher following iontophoretic administration compared to intravenous.84 In ECT, electrical pulses open up transient pores in the cell membrane and allow influx of chemotherapeutic drugs into the cytosol. Bleomycin combined with ECT has shown efficacy in vitro in reducing the activity of human conjunctival melanoma cell lines.85 A simulation on a 3D mathematical model of the eye suggested that ECT can be safely applied to treat intraocular tumors,86 but neither animal nor human studies have yet to be attempted.
Although it is likely that targeted therapies like HIFU, iontophoresis, and ECT will be available for human trials for many types of cancer soon, these therapies would need to be directly compared side by side with plaque brachytherapy in a phase 3 clinical trial in order for their utility in the treatment of uveal melanoma to be considered. Many steps remain in this process.
Conclusion
In conclusion, uveal melanoma is a malignant proliferation of melanocytes within the middle eye. Although advances in the diagnosis and treatment have improved the prognosis of this disease, half of those with uveal melanoma are still at risk of metastasis.51 Uveal melanoma-related mortality was estimated at 31% in 5 years, 45% in 15 years, and 49% in 29 years.6 Further research is warranted to promote earlier identification, particularly in the context of blood biomarkers such as CTCs, ctDNA, cmiRNA to minimize overall tumor burden. The combination of prognostic indicators to create a composite score using AJCC staging, GEP, and chromosome 3 and 8q status also shows promise and warrants further exploration. Studies should also be aimed at testing the efficacy of focused treatments like HFU, iontophoresis, and ECT in uveal melanoma in humans, since these treatment modalities have so far only been explored in animal models. These advancements together would substantially reduce the mortality of uveal melanoma.
Conflict of interest
None of the authors have identified a conflict of interest.
Financial Disclosures
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.