Introduction
Uncertainty is rife in pediatrics. As rapid scientific advances shift previously lethal pediatric illnesses to the realm of chronicity (eg, cystic fibrosis, organ failure, cancer), parents are increasingly faced with the challenge of coping with and, over time, adapting to their child’s uncertain health. Uncertainty in the face of a serious health threat has been described as “probably the greatest single psychological stressor,”1 and in the realm of pediatrics has the potential to impact the parent, the child, or both.2 The resultant consequences have been demonstrated among parents of children with cancer in associations between perceptions of uncertainty and depression,3–5 anxiety,3–8 and symptoms of posttraumatic stress disorder.5,8–10 Such evidence along with the impact on medical decision-making has identified management of uncertainties as a core component of patient-centered cancer care.11
Parental uncertainty in pediatrics is not limited to cancer. Sustained perceptions of uncertainty have been described among parents of children with a variety of chronic conditions, particularly unpredictable conditions such as epilepsy,12,13 autism spectrum disorders,14–18 pediatric rheumatic disease,19–21 and asthma.20,22,23 Perceptions of u ncertainty have also been described among parents adapting to their child’s solid organ transplant.24–26 The ubiquitous nature of uncertainty, cross-cutting numerous medical conditions and psychological outcomes,27 highlights its importance as a priority for research and clinical care. A shift from health care providers’ tendency to suppress the reality of medical uncertainty to acknowledgement and discussion with patients is needed to support informed decision-making.28 Understanding of parental perceptions of uncertainties related to their children’s conditions in clinical and research settings will aid in development of communication interventions and psychotherapeutic strategies aimed at specific domains of uncertainty important to parents.
The Parent Perception of Uncertainty Scale (PPUS),29 which is the most frequently used scale according to a recent meta-analysis of studies of uncertainty in pediatric chronic illness,2 was developed for parents of acutely hospitalized patients, rather than patients living with chronic conditions.30 Weak factor loadings, issues of cross-loading in the initial publication,28 and discrepancies in factor structure reported in a subsequent article4 raise questions about the validity of PPUS. Poor internal consistency of 2 PPUS subscales resulted in unusable data in studies of parents of children with undiagnosed conditions31 and autism spectrum disorders,14 suggesting limitations to its reliability as well. Moreover, the 4 domains of the PPUS (ambiguity, lack of clarity, lack of information, and unpredictability) are consistent with current theoretical understanding of sources of uncertainty in health care32; structuring the domains according to substantive issues of uncertainty—ie, the outcomes of uncertainty—is of arguably greater clinical utility. As such, n ovel measures are needed .
The objective of this research was to develop and validate a novel scale assessing domains of parental perceptions of uncertainties in the context of caring for a child with a chronic medical condition. Because parents of children with intermittently unpredictable conditions are at higher risk for negative psychological outcomes,33 perceptions of uncertainty may be particularly salient and important to understand among parents of children without a diagnosis . For this reason, the scale was applied in 2 distinct populations of parents with children who have undiagnosed medical conditions. Data from 2 similar studies34,35 exploring the role of perceived uncertainty in a parent’s ability to cope with and adapt to their child’s chronic undiagnosed condition were used to identify an interpretable factor structure among the indicator items to be used as a measurement model. Data from a third study offering genome sequencing to parents of children with undiagnosed neurodevelopmental conditions36 were used to determine the extent to which the measurement model would be supported across all 3 data sets.
Methods
An initial scale was drafted from a narrative literature review on uncertainty in the context of chronic health conditions, with attention paid to evidence from the parental perspective and concepts from the spread of uncertainty theory.37 This theory embodies the desired dimensionality for the Parental Uncertainty About a Child’s Health Scale (PUCHS), which maps onto health-related outcomes by framing the impact of sustained medical uncertainty on parental cognition and behavior within 5 domains. The spread of uncertainty theory delineates parental uncertainties about illness origin, evaluation of potential treatment options, and survival and quality of life. A contemporary conceptual taxonomy of uncertainty in health care designates these dimensions disease-centered uncertainties that reflect the parent’s perception of medical knowledge.32 The PUCHS denominates these diagnostic, prognostic, and therapeutic uncertainties. The spread of uncertainty theory also describes parental uncertainties related to unfamiliar environments and consequences for the parent (eg, stress on the spousal relationship, limitations on planning for the future), which are designated patient-centered uncertainties in the personal domain of the taxonomy and reflect aspects of the extramedical experience of parenting a child with a chronic condition. The PUCHS denominates these social and familial uncertainties.
Clinical evidence from cohorts of parents whose children were enrolled in intramural studies at the National Institutes of Health (NIH) suggested that disease-centered parental uncertainties encompass not only diagnostic, prognostic, and therapeutic issues, but also reproductive issues.38,39 In addition, patient-centered parental uncertainties encompassed familial and social issues, as well as existential issues regarding the meaning and purpose of the child’s life according to these parents.38,39 Five parents of children with chronic undiagnosed conditions enrolled in a research study at the NIH were recruited to complete the scale and participate in a follow-up, cognitive interview to assess their understanding of each item, the relative value of the items being assessed, and the ease of use of the scale. Revisions to improve the clarity by simplifying the language of several items were made based on the interviews. With a readability score of 61.9 according to the Flesch-Kincaid readability assessment (corresponding to an 8th or 9th grade reading level), the final draft of the PUCHS was administered to an additional 10 parents of children with undiagnosed disorders enrolled in an exome sequencing study at the NIH to determine the cause of their disorders; comments were solicited in writing and via cognitive interviews. Responses demonstrated substantial variation in uncertainty perceptions, with the exception of the indicators for the existential domain: parents responded that they either strongly disagreed or were unsure about their existential certainty, and they uniformly found the items to be of very little importance. Although indicators for this domain were included in the subsequent administration of the PUCHS based on parental feedback that the items were important earlier in their child’s life, there was initial evidence to suggest that these indicators may perform differently from the other domains of uncertainty in the PUCHS.
Participants
Three studies provided the data for the analyses reported herein. Informed consent was obtained from all participants prior to participation. The first (n = 93) was conducted within the membership of Syndromes Without a Name -USA, U.R. Our Hope, and In Need of a Diagnosis from June to November 2013, and was approved by the institutional review board at the National Human Genome Research Institute.34 The second study (n = 56) was conducted in the United Kingdom, Australia, and New Zealand from June to October 2013, and was approved by the Griffith University Human Research Ethics Committee.35 All participants in both studies completed the PUCHS as part of an online anonymous survey. Individuals who were older than 18 years and a parent (biological or adoptive) of a child with a medical condition that had remained undiagnosed for more than 2 years were eligible to participate in either study. In both studies, “undiagnosed medical condition” was defined as involving 2 or more abnormalities that may have been genetic in nature but an underlying cause or diagnosis had not been identified. Given the relatively small samples and the similarity in participant demographics and cross-sectional design, these 2 data sets were combined (sample A) to develop a measurement model.
The third dataset (sample B) originated from a study conducted in the United States from June 2013 to May 2018, which was approved by Western Institutional Review Board and subsequently the institutional review board at the University of Alabama at Birmingham.36 Participants completed the PUCHS as a part of a paper questionnaire. All responses were entered by research staff into an online database and then checked for accuracy by a second staff member. Individuals were eligible to participate in this study if they were the parent of a child with an undiagnosed neurodevelopmental condition (ie, intellectual disability or developmental delay). This sample was used to test configural invariance of the measurement model.
Measure
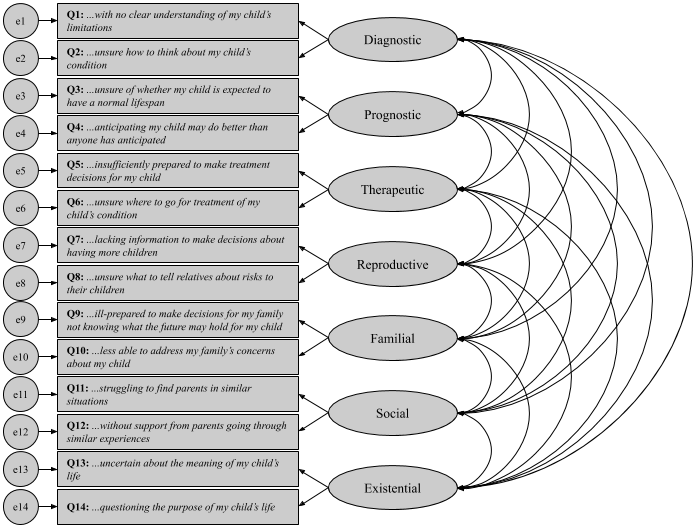
The first iteration of the PUCHS comprised 14 items posited to capture 7 domains of uncertainty perceptions: diagnostic, prognostic, therapeutic, reproductive, familial, social, and existential. As shown in Figure 1, response options for each of the Likert items assessing perceptions of uncertainty range from “strongly disagree” (1) to “strongly agree” (5). Note that the stem can also be “My child’s diagnosis of [condition] leaves me…” Higher scores indicate participants perceive greater uncertainty related to their child’s condition.
Statistical Analysis
Based on the literature and clinical experience described above, an initial factor structure for the PUCHS with 7 domains and 2 indicator items defined to represent each of the domains was hypothesized. Descriptive statistics were used to refine the hypothesized model. Using the refined model as a measurement model, a confirmatory factor analysis was conducted using the following fit statistics: normed chi-square (χ2/df) goodness-of-fit, the comparative fit index (CFI), the Tucker-Lewis Index (TLI), the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). The model was deemed to be supported by the data if the following were satisfied: normed χ2 < 3 (dependent on sample size), CFI > 0.9, TLI > 0.9, RMSEA < 0.1, and SRMR < 0.08.40 Additionally, construct validity for each of the proposed domains of uncertainty was assessed in terms of convergent validity (standardized loadings >0.5, construct reliability >0.7, average variance extracted >0.5) and discriminant validity (average variance extracted > squared correlation coefficient).40 Mplus (version 8.3) was used to obtain weighted least squares mean and variance-adjusted estimates of categorical response variable loadings in the confirmatory factor analysis models and conduct the analyses.
Results
Demographics
The data comprising sample A came from 2 separate studies assessing uncertainty perceptions as they relate to predictors (eg, personality traits) and the outcome of psychological adaptation to parenting a child with an undiagnosed chronic condition involving multiple organ systems. Individuals enrolled in the former study (n = 93) were predominantly White (95%), married (77%) biological mothers (93%) of the affected child. The children were mostly female (58%) and had a mean (SD) age of 8 (5.2) years.34 Individuals enrolled in the latter study (n = 56) were also predominantly married (75%) mothers (98%); race and ethnicity were not collected. The children were mostly younger than 5 years old (39%) or between 5 and 10 years old (29%).35 The data comprising sample B (n = 417) came from a third study assessing uncertainty perceptions in the context of caring for a child with an undiagnosed neurodevelopmental condition. Individuals enrolled in this study reported identifying as American Indian or Alaska Native (5%), Asian (2%), Black or African American (10%), White (80%), other (1%), or multiple races and ethnicities (1%). Participants were predominantly non-Hispanic (97%), and all were biological mothers of the affected child. Marital status was not collected. The children had a mean (SD) age of 8 years.36 No demographic variable was associated with any significant differences in uncertainty.
Initial Measurement Model Analysis
Descriptive statistics from sample A were used to refine the proposed 7-factor model (Figure 2). The 2 items theorized to load onto existential uncertainty (Q13, Q14) were strongly correlated (Spearman r = 0.91) and neither of these items were strongly correlated with any of the other indicators (Spearman r < 0.29). Consequently, these items and their associated construct were dropped from the measurement model. In addition, 1 item (Q4) was insufficiently correlated (Spearman r < 0.18) with any other item to be included in further analysis. Because the future-oriented wording of the remaining item initially posited to load onto prognostic uncertainty (Q3) was similar to that of the indicators for familial uncertainty (especially Q9), it was included in subsequent analyses as an indicator of familial uncertainty.

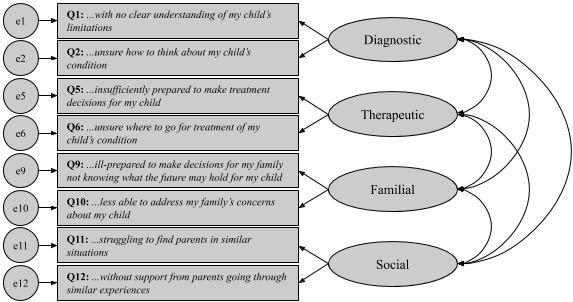
A confirmatory factor analysis was used to determine whether the data supported the resulting measurement model consisting of the 5 constructs (diagnostic, therapeutic, reproductive, familial, social). In the resulting model, Q7 had a communality of 0.33, which fell below the standard threshold for inclusion (>0.5); the item was therefore dropped. Given that the reproductive domain of uncertainty could not be identified sufficiently by a single indicator, the reproductive construct (and consequently Q8) was subsequently dropped as well. Modification indices for the resulting 4-factor measurement model indicated that Q3 cross-loaded with the diagnostic domain. A qualitative review of Q3 revealed that the item was worded in such a way that it could measure either the familial or diagnostic construct. It was omitted from the measurement model resulting in the model shown in Figure 3, which was supported by the data in sample A (normed χ2 = 2.3, CFI = 0.99, TLI = 0.97, RMSEA = 0.095, and SRMR = 0.035). All resulting weights (Table 1) and correlations (Table 2) were significant and positive. All communalities were greater than 0.7, and modification indices were acceptable. For each of the constructs, the reliability was greater than 0.7 and the average variance extracted was greater than 0.5 (Table 1). Additionally, the squares of the correlations between constructs were less than the average variance extracted of the corresponding constructs, and convergent and discriminant validity were satisfied. Thus, structural validity was satisfied per the prespecified criteria.
_an.png)
Configural Invariance Analysis
While the measurement model in Figure 3 was developed using the data from sample A and yielded an adequate fit, it was important to determine that the fit was not specific to sample A. Sample B represented an independent data set that could be used to determine whether the measurement model in Figure 3 could apply to measure uncertainty in other similar clinical settings. The measurement model in Figure 3 was supported by the data from sample B (normed χ2 = 4.7, CFI = 0.99, RMSEA = 0.094, TLI = 0.97, and SRMR = 0.023); the overall model fit was deemed acceptable given the large sample size. All resulting weights (Table 1) and correlations (Table 2) were significant and positive. All communalities were greater than 0.7, and modification indices were acceptable. For each of the constructs, the reliability was greater than 0.7 and the average variance extracted was greater than 0.5 (Table 1). The 4-factor measurement model also satisfied convergent and discriminant validity. This indicates that full configural invariance was supported for the 4-factor model of parental uncertainty shown in Figure 3 for sample A and sample B. Median, SD, and standardized loadings for the 8 individual items, as well as the average variance extracted and reliability for each of the 4 first-order domains of parental uncertainty in the final model, are shown for the 2 samples separately in Table 1.
Discussion
The PUCHS seems to be a valid and reliable psychometric measure of perceptions of uncertainty among parents of children with undiagnosed medical conditions irrespective of the clinical context in which they present. The results demonstrate that a 4-factor model (Figure 3) consisting of 8 indicator items was supported across 2 samples comprising data from various developed nations and distinct realms of undiagnosed disease. Though the normed χ2 in sample B was slightly higher in magnitude than traditional cutoffs for acceptable model fit, inferences based on this statistic should be made with caution given its sensitivity to sample size.41 Based on the other fit indices and indicators of validity, the 4-factor model including diagnostic, therapeutic, familial, and social uncertainties was found to be acceptable. Participants reported high perceptions of uncertainty overall, which is consistent with previous research in parents of a child with an undiagnosed medical condition.31,38 The relatively high level of perceived uncertainty in the social domain makes clinical sense in that fostering connections with parents in similar situations is more challenging without a diagnosis.26 It remains for future application to determine whether this is specific to the realm of undiagnosed disease or whether it pertains to chronic pediatric conditions more generally.
The PUCHS captures disease-centered uncertainties parents face in the context of medical decision-making on behalf of their child and patient-centered uncertainties they must manage on a daily basis caring for their chronically ill child. Disease-centered uncertainties are understood to encompass diagnosis, prognosis, and treatment. However, the items developed to capture prognostic uncertainty—“unsure of whether my child is expected to have a normal lifespan” (Q3) and “anticipating my child may do better than anyone has anticipated” (Q4) —did not generate data that was workable with the rest of the scale. There are many potential explanations, including most likely that the wording of Q4 was problematic because it embodied a cognitive appraisal: rather than capturing the raw perception of uncertainty regarding the anticipated quality of life for the child, it incorporated a positive appraisal (ie, tantamount to hope) confounding responses from parents completing the scale who might have appraised the uncertainty negatively and experienced it more as fear. This is rather unique for this item and could explain its inadequate association with the rest of the indicator items. In addition, it could be that the parental experience of prognostic uncertainty is more complex and multifaceted than survival and quality of life than science might predict. For example, perceived uncertainty about their child’s prognosis may encompass questions of disease course (eg, whether there will be sudden changes or whether the severity will plateau). It is important to note that this in no way indicates that prognostic certainty is not a concern for parents whose affected children have no diagnosis. Rather, it suggests that these 2 indicator items as written were simply inadequate to capture the cognitive and emotional experience of grappling with a child’s uncertain future.
The items developed to capture parents’ perceptions of patient-centered uncertainties about reproductive decision-making (Q7) and risks for relatives (Q8) were also eliminated from the final iteration of the PUCHS. As with the items for prognostic uncertainty, it is likely that these 2 items were not exhaustive in their measurement of reproductive uncertainty (eg, reproductive uncertainty may also pertain to risks for the affected child’s children, which might not have been understood as included in risks for relatives). It is also possible that the future-oriented nature of the wording impacted the responses to Q7 (as well as Q3 and Q4), and that the parents responding to the scale were more focused on the immediate challenges they were facing, eg, what the implications for their family will be and whether they will be able to find needed social support.
The items posited to assess existential uncertainty—“uncertain about the meaning of my child’s life” (Q13) and “questioning the purpose of my child’s life” (Q14) —were eliminated from the PUCHS in early model refinement because there were many indications that these items were performing differently from the rest of the scale. For example, this was the only domain for which parents perceived more certainty than uncertainty. The indicators of existential uncertainty were highly correlated with each other but not with other items, suggesting they are measuring the same concept and that existential uncertainty is an independent construct from the other domains. Accordingly, these items were excluded from the model, and the resulting model was supported by the data from the 2 distinct samples. Although the existential items were removed from the PUCHS, responses from the parents are telling: parents perceive high certainty about the meaning of their child’s life, and the relative lack of certainty about the condition is unrelated to their assessment of the value of their child’s life. Further research may be warranted with a scale other than the PUCHS on assessment of the existential meaning of an affected child’s life with or without a diagnosis.
Limitations and Future Directions
While this study provides strong evidence for the PUCHS as a measure of parental perceptions of uncertainty, extrapolation of the findings presented here is limited primarily by sample. The homogeneity of the samples in race, ethnicity, parental gender, and biological relation to the child limit the external validity of these findings. Additionally, the PUCHS has only been shown to be valid and reliable among parents of children with undiagnosed medical conditions. Administration of the PUCHS in more diverse populations and contexts will continue to elucidate the nature and behavior of perceptions of uncertainty as they relate to clinical outcomes. One additional limitation of this validated iteration of the PUCHS is that it encompasses only 4 domains of parental uncertainty with only 2 indicators per domain. Though this brief version captures clinically important uncertainties about diagnosis, treatment, familial, and social implications of caring for a chronically ill child (and has an added benefit of requiring little time to complete), future research is likely warranted on the development and validation of additional items to capture these domains of uncertainty more completely as well as additional domains of parental uncertainty about the health of a child (eg, prognostic, reproductive). Nevertheless, the 4 domains of the PUCHS, which discriminate among disease- and patient-centered outcomes of uncertainties, will prove more helpful than existing measures in identifying parental needs and facilitating clinical management.32
Practice Implications
Mishel42 theorized that uncertainty management in chronic illness is vital to mitigating negative consequences. Beyond its demonstrated relationships with parental anxiety and depression, parental uncertainty has been shown to impact the child’s psychological functioning.2 Moreover, high levels of uncertainty can impede information management (eg, as in avoidance coping) and bias decision-making, 2 critical processes in the context of caring for a child with a life-threatening condition. While the literature on interventions remains modest, correlational studies have suggested promising strategies including increasing parental sense of mastery6 or feelings of control.38 Additionally, a number of interventions have been pilot-tested: reduction of parental uncertainty following diagnosis of type 1 diabetes,43 psychoeducation of mothers following a cancer diagnosis,44 and acceptance and commitment therapy for parents of children with cancer.45 Ultimately, common to each of these interventions is boosting the parent’s self-efficacy in responding to the health threat, something health care providers can achieve by helping parents recount coping mechanisms that have proved effective for them in the past and encouraging them to engage available resources.
When considering interventions, it is important to distinguish the various types of uncertainties that patients and families experience given that these uncertainties differ in their reducibility. For example, aleatory uncertainty (also known as probability or inherent randomness) is irreducible by additional information, whereas epistemic uncertainty (eg, ambivalence) is reducible and requires different management strategies.32 Social uncertainty related to identifying parents in similar situations is a prime target for interventions: parents can be connected with advocacy organizations or support groups for community connection or with individual families in similar circumstances for interpersonal connection. On the other hand, therapeutic uncertainties arising from the ambiguity and complexity of available evidence are often less reducible, and may be better managed through modification of cognitive appraisals and empathic support.
It should be emphasized that perceptions of uncertainty are known to have paradoxical effects. For example, uncertainty can result in fear or hope, depending on the cognitive appraisal,46,47 although the outcomes of uncertainty depend on several additional factors.48 Fear of an uncertain health threat can prompt a parent to preemptively engage in a health behavior for their child (eg, frequent monitoring, unnecessary care) to reduce uncertainty or to avert a health behavior because acting on a threat makes it more real.49 Because the outcomes of uncertainty depend on cognitive appraisals, personality traits, available coping resources such as health care professionals and social support,50 and other patient resources, managing uncertainty does not necessarily entail reducing it. Instead, assessing how the uncertainties perceived by the parent relate to coping and adaptation to their child’s condition will likely prove a more effective strategy.
Conclusions
The PUCHS is a promising psychometric of uncertainties related to parenting a child with a chronic medical condition, particularly when the uncertainties perceived are profound as is the case in the realm of undiagnosed disease. Albeit not fully comprehensive of every type of uncertainty that may be perceived by parents of children with a given condition, the PUCHS has been shown to be a valid and reliable measure of 4 types of uncertainty that are common across pediatric illness: what a diagnosis means, what the best therapy is, what the implications for the family are, and who the parent can turn to for help in understanding their situation. Quantifying these perceptions promotes understanding of outcomes of uncertainty and communication of salient uncertainties between parents and health care providers. Effective management of these uncertainties—a core function of patient-centered care—is consequential for all stakeholders.
Sources of Funding
This work was supported by the Intramural Research Program of the National Human Genome Research Institute at the National Institutes of Health.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Acknowledgements
We thank the parents who participated in the pilot testing and interviews. Mr. Umstead thanks Dr. Catherine Cohn for teaching him how to think critically and inspiring in him a love for problem solving.