Introduction
Social determinants of health have a profound influence on health outcomes. Housing status is one such relevant determinant. Among those living with HIV, a disproportionate number are also experiencing homelessness, with an estimated 8% of people living with HIV/AIDS (PLWHA) lacking housing.1 Because of advancements in treatment, HIV can be managed as a chronic condition with the use of combination antiretroviral therapy. Antiretroviral therapy reduces viral load to untransmissible levels with the appropriate adherence, preventing the progression of HIV to AIDS and significantly reducing mortality.2,3 However, homelessness may pose a barrier to the optimal levels of combination antiretroviral therapy adherence to maximize health outcomes.4 As such, differences in HIV outcomes may occur as a result of reduced adherence levels.
Differences in adherence levels among PLWHA due to housing status should be set within the context of the socioecological model framework. This framework explains that multilevel factors modify the transmission and treatment of HIV. The multiple levels encompass individual behavioral decisions, social factors, and structural factors.5 Housing status, a structural factor, strongly influences lower levels of factors such as an individual’s sociocultural environment and personal decisions. Thus, the demographic descriptor of homelessness becomes more than just a descriptor of someone’s housing status, but also indicates the presence of other common environmental and demographic features that uniquely modify individuals’ health decisions and outcomes.

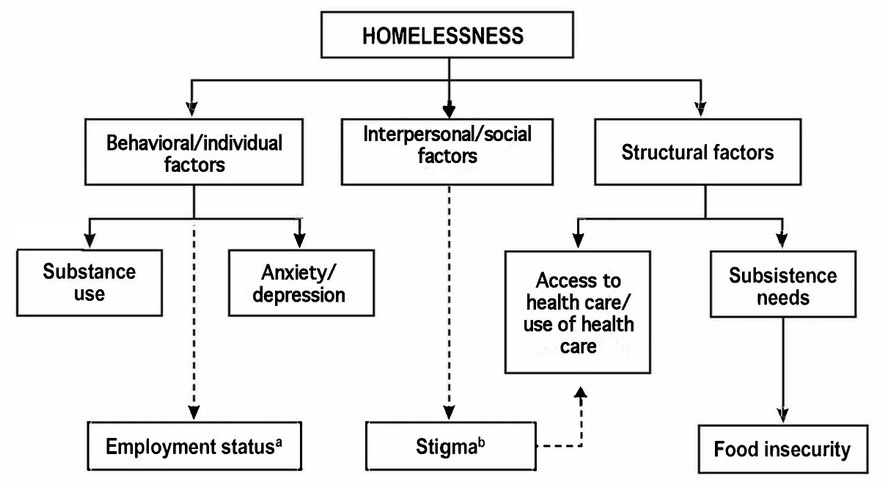
There are various factors of homelessness within the socioecological framework contribute to the overall effect. Figure 1 provides an overview of co-related factors; these levels can be grouped into behavioral or individual factors, such as substance use, employment status, and mental health status; social factors, such as stigma; and structural factors, such as access to subsistence needs and access to health care. In the socioecological model, the structural factor of homelessness creates the context that greatly determines interpersonal/social factors and behavioral/individual factors.
The impact of homelessness on treatment adherence is a multifactorial phenomenon. Individual and behavioral factors of PLWHA can affect overall treatment adherence levels and health. People experiencing homelessness are more prone to binge drinking, using both noninjection and injection drugs, and smoking than individuals with housing.6–8 Additionally, individuals experiencing homelessness are more likely to have depression, thus also modifying behaviors.9 Depression and psychological distress have been associated with reduced HIV care retention.8 Nationally, about 53% of people experiencing homelessness were found to be formally employed.10 Individuals with employment and unclarified housing status (housed vs unhoused) are able to achieve higher levels of health with more consistent access to health care and financial stability.11 Other levels of the socioecological model can impart effects on adherence levels as well.
People living on the streets or in shelters lack privacy in their social lives. This falls under the social and structural factors related to homelessness displayed in Figure 1. HIV stigma has been found to be significantly higher among people who are homeless or unstably housed, where stigma is the experience of avoidance, blame, or verbal abuse in relation to one’s HIV status.12 Without a private location to take their prescriptions, people may avoid medication altogether, fearing inadvertent disclosure of their HIV status.13 PLWHA also face external stigma on the basis of their housing status from individuals with housing. Dual stigmatization contributes to community rejection of the needs of PLWHA experiencing homelessness, thus hindering the development of integral health and housing services for PLWHA who are homeless.14 This reduces the accessibility of necessary health care for people experiencing homelessness. In a qualitative study discussing various modes of antiretroviral therapies, individuals experiencing homelessness reported that daily oral medication was difficult to take because of the barriers to seeing a physician, getting the prescription, and having it filled.15 Access to health care professionals and treatment is necessary for complete adherence.
Structural factors associated with lack of housing greatly contribute to limited fulfillment of basic subsistence needs. Unmet subsistence needs may include difficulties accessing a bathroom or a place to shower or purchasing clothing or food.16 These basic factors, required for basic human functioning, may be prioritized by people experiencing homelessness over other needs such as the management of chronic illnesses such as HIV.17,18 Competing needs act as barriers to individuals facing housing insecurity who are seeking the adequate health care that they require to live healthy lives.
The objective of this literature review was to identify both associations between homelessness and antiretroviral therapy adherence, as well as relationships between other modifying variables associated with housing status and treatment adherence. The findings should be used to inform an understanding of contributing socioecological factors that individuals experiencing homelessness typically face, as well as the association between these contributing factors and housing status with antiretroviral therapy adherence.
Methods
For this systematic literature review, we searched PubMed for English-language articles published from 2000 through January 2023 using the following key words for antiretroviral (anti retroviral agents, anti retroviral, antiretroviral antiretrovirally, antivirals, anti HIV agents), therapy (therapeutics, therapies, therapy, therapy, antiretroviral therapy, highly active), adherence (adherence, adherance, adhere, adhered, adherer, adheres, adhering, medication adherence, treatment adherence and compliance), homelessness (ill housed persons, ill housed, homeless, homelessness, housing instability), and HIV (HIV infect*, HIV infections). The OR operator was used for syntax and synonyms within parentheses, while the AND operator was added between each term. The filter of adult was applied. This search method resulted in 49 preliminary articles.
Eligibility criteria included articles with a term for homelessness and an outcome of antiretroviral therapy adherence. Articles using the provision of housing as an intervention to influence adherence were also included. Articles that also explored the impact of other modifying factors (eg, substance use, mental health, education level) were included as long as the samples were stratified by housing status or among a sample of individuals experiencing homelessness. Titles and abstracts were adjudicated for inclusion by an investigator with expertise in HIV and housing, of which 10 were deemed relevant. Two additional articles were added after parsing the references of included articles.
Results
Summaries of included articles are provided in Table 1
General Demographics
Across all included studies, HIV-positive individuals experiencing homelessness were predominately composed of male respondents, with a large proportion of the samples being African American. A general summary of participant demographics for these studies is provided in Table 2. Of participants without housing, Cassimatis et al26 found that 34% of those were living temporarily with friends, while less than 5% were living outdoors or in a shelter. In the implementation of the Housing and Health Study, Kidder et al28 determined that 62.1% of participants were temporarily doubled up, which is defined as temporarily sharing housing with others, followed by having temporary housing (23.6%), or residing in a homeless shelter (15.5%). Moss et al20 found that 9% of participants were residing on the street or in a shelter at their baseline visit. Cassimatis et al26 and Kidder et al22 found that individuals experiencing homelessness were less likely to be employed than participants with housing. However, the relationship between employment status and treatment adherence was not explored in any of the identified articles. Likewise, many populations experiencing homelessness had a history of substance use.22 People experiencing homelessness have been found to need more mental health counseling compared with counterparts with housing.22
Housing Status and Antiretroviral Therapy Adherence
Housing status has a strong influence on a multitude of relevant factors for HIV outcomes, most notably treatment adherence. In many studies, participants were considered to be experiencing homelessness if they answered “yes” to living in a shelter for those without housing, car, single-room occupancy hotel, on a street, or in another public space.6,9,19,22,27 Studies had varying periods related to the classification of housing status, ranging from 30 days prior to the study to up to a year. Adherence levels can vary over the period measured, slightly modifying the studies’ reliability, with some studies confirming such relationship between homelessness and adherence over various periods from 2-day adherence to week-long adherence.22,24 Adherence generally was defined as the percentage of medication doses taken as prescribed for all antiretroviral therapy medication doses in a set time frame prior to the study interview. While studies were relatively similar in how they defined and measured housing status, adherence measures varied significantly in the periods that they measured, from 1-day adherence to month-long adherence.
The Medical Monitoring Project is an annual, nationally representative cross-sectional study conducted by local health departments in partnership with the Centers for Disease Control and Prevention (N = 669), with a predominantly male (74.5%) and Black (49.5%) sample and a median age falling in the 40- to 49-year age range.6 Homelessness was defined as an individual being homeless for any period of time within the past year, while antiretroviral therapy adherence was assessed by a 3-item scale on adherence during 30 days prior to the interview. Adherence was measured in the past 7 days using the AIDS Clinical Trials Group adherence questionnaire and self-reported prescribed and missed antiretroviral doses to compute adherence percentages. Viral loads and CD4 counts were assessed by medical record abstraction. Per recommendations from the Department of Health and Human Services, monitoring of viral load, CD4+ cell counts, and antiretroviral drug–related adverse effects should be completed for all PLWHA.29 Wainwright et al6 found that in this sample, homelessness was associated with a reduced likelihood of 100% dose adherence over the past month when compared with counterparts with housing (prevalence ratio, 1.37). This analysis suggested that unmet need for housing services or shelter was 3.13 times more prevalent among people facing homelessness as opposed to those with stable housing. Self-reported unmet housing needs from participants further magnifies the justification for improved housing resources in the United States.
Of 5 studies identified as being related to medication adherence in a systematic review by Leaver et al,27 all of them had demographic makeup of at least 70% male participants and of the studies that identified race and ethnicity, 43% to 65% were African American in the samples. All of the articles found a significant positive relationship between improved housing stability and adherence.27 Housing status was similarly defined as living in a shelter, single-room occupancy residential hotel, or a public place such as a car or street, although in some cases, housing stability was considered a frequency of change in residence. Studies had variable adherence reporting methods. One of the studies that analyzed a predominantly African American sample (65%) with relatively split risk factors among those who used injection drug (27.5%), men who have sex with men (28.3%), and heterosexual participants (27.5%), found that homelessness was associated with a lack of receiving antiretroviral therapy in the first place. One study sample was composed of participants who had a history of homelessness or living in a shelter and found there were significant univariate and multivariate associations to poor self-reported adherence, where adherence was either classified as greater than or less than 90% adherence. Over all of the studies, the systematic review determined that long-term housing was significantly associated with better adherence to combination antiretroviral therapy (75% vs 42%). There was a 1.38 increased likelihood of poor adherence among people with a history of homelessness compared with those who had not experienced homelessness.27 Common identified weaknesses included that many of the studies used a measure of adherence that had low validity and overestimation, with some studies failing to collect clinical indicators to support validity of self-reported adherence levels.27
Housing instability adversely impacts particularly vulnerable populations. Cassimatis et al26 performed a retrospective cohort study of pregnant, HIV-positive individuals (N = 232), among which the median age was 26 years and 80.2% were White. Housing instability was assessed by a clinical social worker and classified as experiencing housing instability if one was staying with family or living in transitional housing, treatment program, shelters, outdoors, in a car, hotel, or was incarcerated. CD4 counts were measured, and adherence was measured by the percentage of those who had missed 5 antiretroviral therapy doses or more.26 The study found that housing instability, when compared with housing stability, was significantly associated with lower adherence (adjusted odds ratio [AOR], 2.09).26 Those experiencing housing instability were younger and less likely to be employed or have a higher education level compared with those who were housing secure. In addition to lower adherence levels, those facing housing instability had increased odds of detectable viral load at delivery, in contrast to counterparts with housing, furthering the risk of perinatal HIV transmission. The housing status of an individual thus can have generational consequences. An individual’s housing status can derail their ability to maintain successful treatment of their HIV disease.
Substance Use, Homelessness, and Adherence
Among individuals with common identifying characteristics and risk factors for poor HIV outcomes, adherence was similarly influenced by housing status. Surratt et al24 studied a sample of HIV-positive participants with substance use disorder, of which the mean age was 45.8 years, 59.2% were men, and 61.9% were African American. Housing insecurity was described as lack of adequate housing over the last 3 months. The study inclusion criteria indicated that those who used drug substances had either used cocaine or heroin 12 or more times in the past 3 months. Adherence was measured using self-reporting and the AIDS Clinical Trials Group adherence questionnaire. Adherence was grouped by adherence percentages. CD4 count and viral load were self-reported. Surrat et al24 concluded that among HIV-positive participants with substance use disorder (N = 503), food and housing insecurity was significantly associated with lower 7-day antiretroviral therapy adherence levels when compared with participants with stable housing and food (β = −0.062, P < .04). Of those experiencing food and housing insecurity, only 40.4% self-reported having good health. Additionally, participants without food and housing security were more likely to divert their antiretroviral therapy medication than those with housing security. Those who diverted medications were less likely to be adherent when compared with those who did not divert their medication (β = −0.227, P < .01).24 Among participants with substance use disorder living with HIV, there were competing interests of their current addiction and their attention to managing their chronic illness through medication. The result of conflicting needs may result in the selling of their medication, culminating in reduced adherence and worse health outcomes.
In a similarly aged (mean, 43.4 years), predominantly African American sample (93.75%) composed solely of men, homelessness was defined as living in a shelter, care facility, or on the street, while substance abuse was defined as having injected drugs within the past year.9 Drug use was further stratified into use of opiates, cocaine, or marijuana in the last week. Individuals experiencing homelessness or marginal housing had greater mean years of drug and alcohol use than individuals with housing. Adherence was self-reported for 1-day adherence, which researchers found to be significantly correlated with mean viral load over 6 months. Additionally, blood samples were taken to measure viral load and CD4 counts. In this study, Waldrop-Valverde and Valverde9 found a nonsignificant positive relationship between housing status and adherence among those with substance use disorder (β = 0.591, P = .37). The nonsignificance of this study may have resulted from a small sample size with insignificant power (n = 42 with housing, n = 16 without housing).9 Additionally, this study was not originally designed to determine the effects of homelessness on adherence, which may further explain the lack of significant findings.
Food Insecurity and Highly Active Antiretroviral Therapy Adherence
Food insecurity is strongly tied to housing insecurity. Those experiencing food insecurity have 62% higher odds of experiencing housing insecurity later and those experiencing housing insecurity have 40% increased odds of facing food insecurity in the future.30 Lack of financial security to obtain housing also contributes to an inability to achieve the appropriate nutritional intake. With this bidirectional relationship, discerning between housing insecurity and food insecurity can be challenging. Challenges that arise with housing insecurity may be the same challenges that arise from facing food insecurity. Indeed, Surrat et al24 grouped housing insecurity with food insecurity because individuals with insecure or no housing are likely to be food insecure.31
Chen et al19 conducted a cross-sectional study among participants who previously experienced homelessness, had been in jail, were predominantly African American (59.6%), and were mostly men (62.4%) (N = 743). Homelessness was defined as self-report of sleeping in a shelter, streets, parks, empty building, bus station, or some other public place. An individual was classified as food insecure if they went without food for 2 or more days. The analysis found that food insecurity was associated with a reduced likelihood of having greater than 95% adherence to antiretroviral therapy when compared with those with adequate nutrition levels (OR, 0.41). The correlation between lower adherence and food insecurity among individuals experiencing homelessness points to the further consideration of unmet subsistence needs and a hierarchy of needs. Subsistence needs are basic housing, water, food, and security needs that are required for human flourishing. Without fulfillment of these needs, individuals may prioritize those needs while overlooking less immediately concerning duties such as taking their medication. Indeed, unmet subsistence needs have been found to have the largest negative population impact on adherence among both women and men experiencing homelessness.17,18 Food insecurity and other unmet basic needs negatively influence adherence levels among individuals experiencing homelessness.
Access to Health Care System/Health Care Professionals/Health Insurance, and Adherence
Lack of a stable home and mailing address can contribute to increased difficulties accessing health care services. These health care services are integral to improved health status and HIV outcomes. Insurance status among individuals experiencing homelessness was the largest predictor of improved adherence. The impact of insurance status had a large effect in the study by Chen et al19 of individuals who had been incarcerated, which determined that while food insecurity contributed to reduced adherence among individuals without housing compared with those with secure food and housing (AOR, 0.41), having health insurance completely mitigated the effect of food insecurity. Those who experienced hunger but possessed insurance had an AOR of 3.05 for taking their antiretroviral therapy in the week prior to incarceration when compared with those who also faced food insecurity but lacked insurance.19
In the Housing and Health Study that included a sample composed of 72% men, who were nearly 100% African American, 42.5% reported having difficulties getting medical care (N = 358).25 Two-day and 7-day adherence were both self-reported and were classified either as 100% adherent or less than 100% adherent over the stated period. CD4 and viral loads were measured but not reported in the study. The cross-sectional study by Royal et al25 found that lacking health insurance was associated with 2-day nonadherence among people experiencing homelessness when compared with those with health insurance (OR, 2.43). Individuals with insurance may more consistently interact with health care professionals who promote the benefits of HIV medications. The HIV Medications Attitude Scale presented participants with a statement regarding HIV medications with a positive or negative perspective. Lower scores on the Attitude Scale correlate to increased negative perceptions about HIV treatment options and health care.25 Indeed, individuals experiencing homelessness who scored lower on the HIV Medications Attitude Scale, in contrast to those with higher scores, had lower levels of adherence (AOR, 0.69).25 The perspectives of people experiencing homelessness on their HIV treatment options and health care contribute to adherence levels.
The perceptions of health care professionals and treatment can be significantly tied to general adherence. In a sample studied by Quinn et al23 composed of individuals experiencing recent homelessness over the course of 18 months (N = 157), adherence was assessed by participants estimating the percentage of total doses they had taken in the past month and then dichotomized as greater than 95% or less than 95% adherence. Those with higher perceived access to health services and lower perceived barriers to care had a higher likelihood of optimal adherence levels in contrast to those with less access and increased barriers (ORs , 1.11 and 0.74, respectively).23 The perceived access to care of participants was measured using a 6-item Access to Care Scale. Barriers to care in the last month was assessed through a 10-item questionnaire about reasons that participants did not get needed medical treatment.23 Because antiretroviral therapy requires a prescription to obtain, optimal adherence levels require that individuals experiencing homelessness have at the very least some minimal contact with health care professionals. Beyond traditionally perceived adherence levels, the number of HIV-positive individuals experiencing homelessness and taking antiretroviral therapy depends on their ability to access health care settings.
Depression/Anxiety and Adherence
Depression and anxiety have been found to be independently associated with reduced antiretroviral therapy adherence irrespective of housing status.32,33 This literature review only analyzed depression and anxiety when mental health status acts as a modifying factor in HIV-positive populations without homes. In the cohort of individuals experiencing homelessness studied by Royal et al,25 depression was based on the 10-item Center for Epidemiologic Studies Depression Scale. The study found greater levels of depression were associated with lower levels of 2- and 7-day adherence levels (AOR, 1.73 and 1.91, respectively).25 The study by Royal et al25 concluded that depression served as a modifying factor contributing to reduced treatment adherence among PLWHA who are experiencing homelessness. Surratt et al24 found that participants without secure housing were more likely to report depression (73.4% vs 40.4%) and anxiety (49.1% vs 17.9%), as measured by DSM-IV-TR criteria, than those with substance use disorder and housing security. However, the study was unable to conclude that depression or anxiety was significantly associated with reduced adherence. Waldrop-Valverde and Valverde9 found a negative association between greater depression levels and adherence (β = −0.079) where Beck Depression and State-Trait Anxiety inventories were used for measurements. However, there was no significant difference in the levels of depression between participants with and without housing in this sample. While one of these studies was able to find an association between depression and housing status and the other between depression and lower adherence levels, neither study was able to conclude that mental health acts as a modifying factor among people experiencing homelessness. Therefore, there is less support for mental health acting as a contributing factor of reduced adherence among individuals without housing. However, the treatment of mental health disorders in populations experiencing homelessness should not be overlooked as a possible intervention to improve overall health outcomes
Discussion

This literature review seeks to place existing findings within a socioecological model. This recontextualization better explores barriers to adherence. Homelessness is a multifactorial phenomenon that shapes the common experiences of individuals. Housing status is not a silo, but is rather modified and influenced by individual factors, interpersonal/social factors, and other structural factors. When adjusting for personal factors that could impact adherence, such as CD4 count, mental health status, and substance use, homelessness was found to still substantially cause increased nonadherence.22,24,26 Individual factors alone are not the sole predictor of treatment adherence levels, but rather found to be modifying factors among those facing homelessness.
Substance use and mental health status were the most prevalent individual factors in regard to antiretroviral therapy adherence.9,18,24,25 Individuals with substance use disorder prioritized different competing needs through the decision to sell or trade (divert) antiretroviral therapy medications for any reason.24 Implied reasons for this diversion included unmet subsistence needs and dependence on drugs.24 Depression and anxiety, already established contributors to reduced treatment adherence, had a similar effect among people experiencing homelessness.25,32 However, only 1 study successfully found a significant association between depression and lower adherence levels in a cohort of individuals to support the modifying effect of depression.25 The other 2 articles were unable to jointly support the relationship between depression and housing status and depression and adherence.6,9 Thus, the status of depression as a modifying factor has less justification in literature.
Likewise, interpersonal/social factors play a role in HIV outcomes. When individuals perceive access to health care as being open and available, they have increased levels of antiretroviral therapy usage.23 The accessibility of health care services for individuals experiencing homelessness requires much more than accessibility for the general population. Individuals without housing experience greater levels of stigma.34 Stigma among health care professionals, including dismissing, dehumanizing, demeaning, and stereotyping patients, has been found to reduce the accessibility of health care services to those experiencing homelessness.35 Much of the ease and accessibility of using health care services depends not only on logistical factors, but also on the openness of health care professionals to compassionately communicate with patients experiencing homelessness. In the absence of positive relationships with health care professionals and in the presence of stigma, those experiencing homelessness avoid health care vital to their well-being.36 Thus, the interpersonal interactions people experiencing homelessness face are relevant to their health outcomes as well.
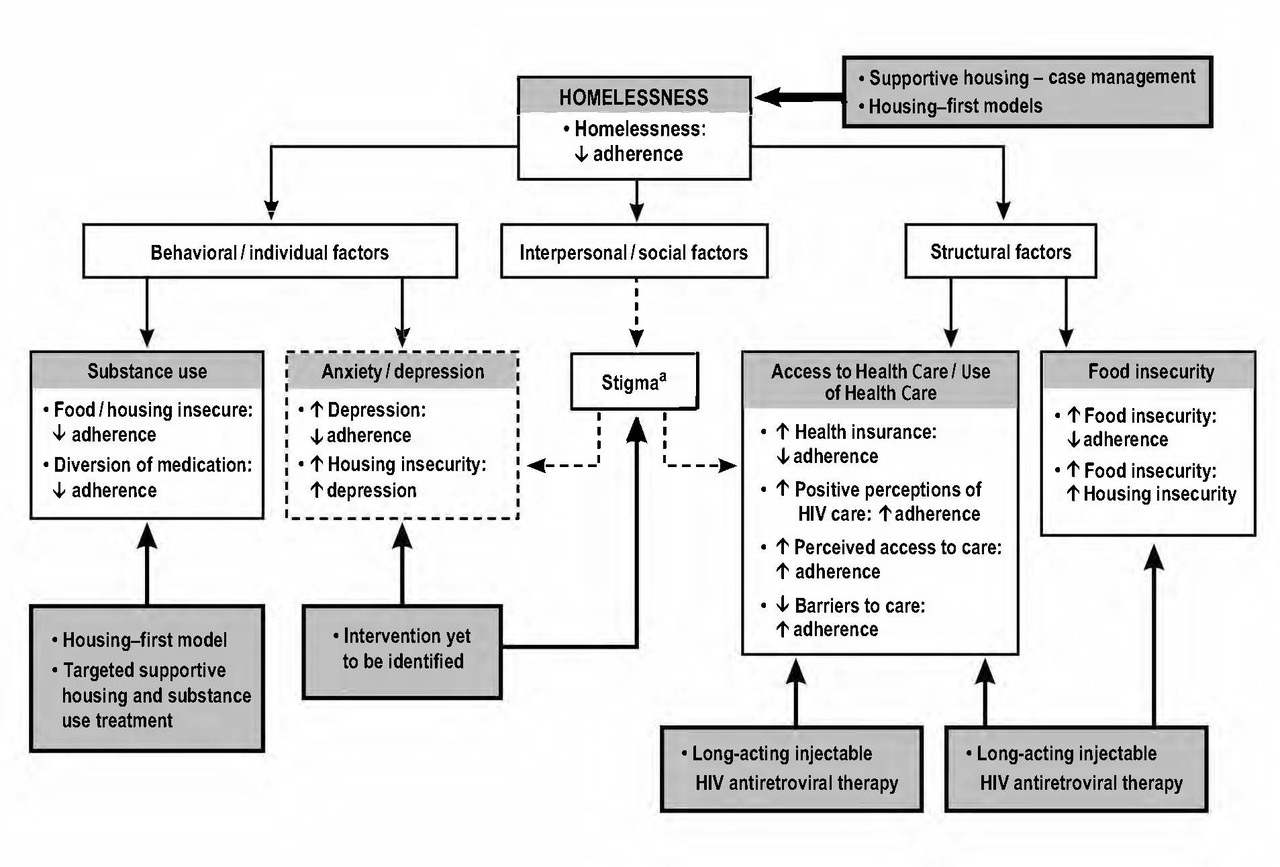
At the structural level, providing housing to those facing homelessness while living with HIV greatly impacts individuals’ treatment adherence levels. The US Department of Housing and Urban Development, through the Housing Opportunities for Persons With AIDS, funds grants for local communities, states, and nonprofit organizations to aid housing-insecure individuals.37 Through federal support, interventions such as supportive housing are enabled. Supportive housing combines providing housing supplemented with case management services.23 In a study of individuals currently enrolled in supportive housing programs, housing satisfaction was significantly associated with increased treatment adherence.23 Contentment with one’s housing situation serves as further proof of the efficacy of improving housing for those experiencing homelessness. Among a cohort of individuals without housing, those who obtained housing throughout the course of the study had an 80% reduction in mortality, likely due to a combination of various factors, from improved adherence to reduced prevalence of other comorbidities.21 One intervention study conducted from 2006 to 2009 evaluated a Housing First program for PLWHA while experiencing homelessness.38 Of study participants, most used drugs and were men. In this study period, 69% of participants achieved viral load. One limitation of this study included a small sample pool.38 Minimal research has looked into the implications of providing housing as an intervention to improve health outcomes among HIV-positive individuals. Further research into the effectiveness of housing-first initiatives is integral in determining how to best support HIV-positive individuals experiencing homelessness.
The provision of housing targets various factors including homelessness, access to health care, food insecurity, and substance use. Housing-first models provide housing without the requirement of those who use substances to prove their sobriety. This type of approach reduces homelessness, and was found to not be associated with an increase in substance use.39 Housing, in conjunction with case management, assists residents in connecting with other resources in a community to meet their food, health care, and other needs. This heightens a person’s capacity to achieve optimal treatment adherence.23 People living with HIV who were provided supportive permanent housing had increased engagement in care and increased viral suppression.40 Providing long-term housing not only addresses the root of homelessness, but also impacts modifying factors related to overall antiretroviral therapy adherence.
Another potential method for improving adherence among people experiencing housing instability may be the use of long-acting injectable HIV antiretroviral therapy. A qualitative study at a drop-in HIV and harm reduction center in Boston, Massachusetts, identified that participants are knowledgeable about antiretroviral therapy adherence and clear about what barriers they have to perfect adherence.15 Most participants said that long-acting injections would be more convenient and that they would not have to worry about their medication being stolen. Many participants discussed housing insecurity as depriving them of secure spaces to store their belongings such as their antiretroviral therapy pills.15 Injectable antiretroviral therapy may be more accessible and tailored to the needs of HIV-positive people experiencing homelessness. Injectables also would help to mitigate internal stigma surrounding HIV.41 A study by Christopoulos et al,42 an early demonstration project in a sample of patients with marginal housing, found the achievement of viral suppression or a 2-log decline in viral load within a month of the first injection. Future research into long-term injectable antiretroviral therapy is required to fully understand the effectiveness and feasibility, but initial results are promising. These long-acting injectable therapies allow for diminished frequency of once necessary health care interactions, from picking up prescriptions at a pharmacy to attending appointments for follow-up regarding antiretroviral therapy regimens.
Further research should be invested into addressing gaps in interventions, particularly targeting stigma and depression among people experiencing homelessness. The literature has identified methods for addressing individual factors, such as substance use, and structural factors, such as housing and access to medication, but little research has been done into interventions aiming to reduce stigma and improve care.43 Stigma from both internal and external perspectives is theorized to influence overall patient levels of depression and attitudes towards HIV treatment, 2 factors that have the capacity to modify adherence levels. Interventions aimed at reducing stigma at the HIV-positive individual’s personal level should be specific to account for unique identities: an HIV-positive individual who uses substances may have a different experience with stigma when compared with a housed person living with HIV. Additionally, investigating how programs can target health professional stigma pertaining to individuals without housing may have the capacity to reduce perceived burdens to accessing care and improve treatment adherence through strengthening support channels for HIV-positive people experiencing homelessness.
Limitations
These literature review findings have several limitations. In some cases, housing insecurity was the primary term instead of homelessness.9,24–26,28 Additionally, variations in definitions of housing insecurity and homelessness limit the reliability of the measures. Therefore, this required a search methodology that encompassed a variety of phrases, for example, homelessness, housing insecurity, and housing status, in order to fully discover all relevant articles. Certain studies used a history of homelessness as a proxy for homelessness.28 Self-reported adherence measures may limit adequate validity; however, the overwhelming majority of the research studies analyzed confirmed validity through biomarkers such as viral load and CD4 cell count.9,20–22,24–26,28 All of the samples were based in the United States. These results are predominantly urban. The majority of sample populations were male-dominated, with limited findings on the impact of gender in relation to homelessness and HIV outcomes. The average age of participants in the studies ranged around the mid to late 40s, with reduced applicability of findings to younger individuals without housing.
Conclusions
A review of the literature suggests that housing status is a significant factor in determining antiretroviral therapy adherence. Homelessness is a multifactorial experience, with various modifying subfactors having immense implications for overall health. While an individual’s housing status has the most profound impact on their treatment adherence levels, the influence of housing status alone cannot fully be isolated from other modifying factors. Individual factors, such as a person’s mental status and substance use, modify a person’s ability to achieve optimal medication levels, while the levels of social stigma that someone faces can disproportionately reduce their ability as well through disincentivizing health care visits. Lack of structural support hinders individuals’ abilities to achieve their most basic living needs and subsequently prevent the maintenance of their chronic HIV conditions. Addressing the basic structural, interpersonal, and individual needs of PLWHA experiencing homelessness is of the utmost importance to improving overall adherence and health outcomes of HIV-positive individuals. Interventions such as the provision of supportive housing should receive increased funding because these programs have the potential to not only improve adherence, but drastically improve the overall well-being of individuals experiencing homelessness. More research into how to target social/interpersonal factors, such as stigma, to improve and comprehensively cover all potential modifiers of adherence is required.
Disclaimers
None reported.
Sources of Support
None reported.
Conflicts of Interest
None reported.