Introduction
Wunderlich syndrome is a very rare condition. It is sometimes referred to as spontaneous renal hemorrhage, wherein there is bleeding contained in the perinephric subcapsular area and there is no history of traumatic events.1,2 This syndrome is usually characterized by the Lenk triad of acute pain over flanks, presence of flank mass, and hypovolemic shock, although these typical findings may not be present in all cases and are not specific to Wunderlich syndrome.3 Wunderlich syndrome is usually caused by kidney malignancies, particularly angiomyolipoma and renal cell carcinoma, which account for approximately 60% to 65% of cases because these tumors are prone to bleeding and bursting.
We report a 41-year-old male who initially presented with flank pain. The patient had hypotension and was found to have a kidney mass, along with subcapsular hematoma, which during further investigation was subsequently removed. This case report intends to highlight the etiology, clinical manifestation, and management of this potentially life-threatening condition.
Case Presentation
A 41-year-old male with no significant medical history presented with progressive right flank pain for 2 weeks prior to admission associated with nausea and 1 episode of vomiting. On further assessment, he denied any fever, chills, or hematuria. His bowel and bladder habits were normal.
At presentation, the patient was hemodynamically stable. There was no significant finding on physical examination except for right-sided abdominal tenderness along with right costovertebral angle tenderness. However, there was no guarding or rebound tenderness.
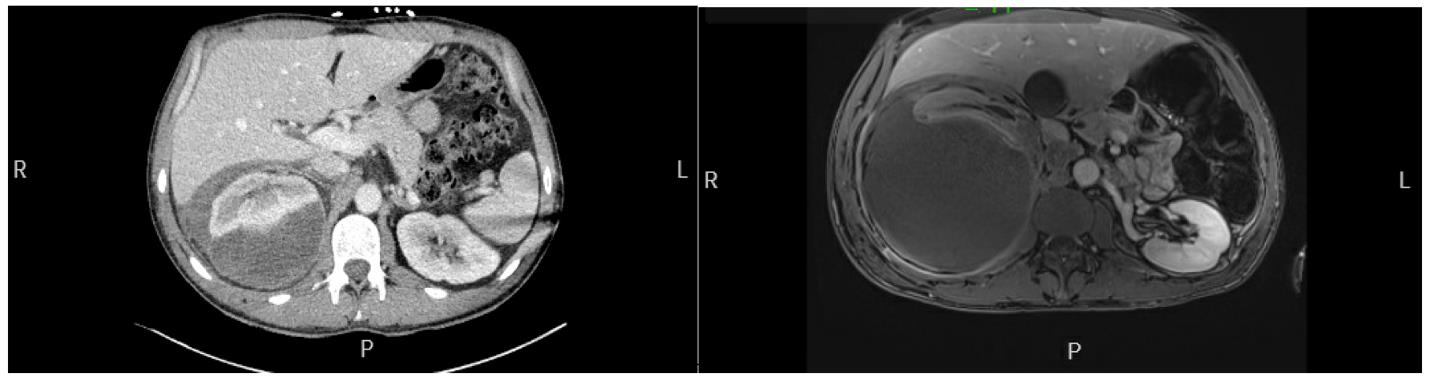
The patient’s laboratory results showed leukocytosis of 14.8/μL (range, 4.0-10.8/μL) and thrombocytosis of 489/μL (range, 145-400/μL) with a hemoglobin level of 14.2 g/dL (range, 12.5-16.5 g/dL). Kidney function was within normal limits, while urinalysis was nonrevealing. As for imaging, ultrasonography of the abdomen revealed a mass in the upper pole of the right kidney. On further assessment, a computed tomographic (CT) scan of the abdomen and pelvis with intravenous (IV) contrast revealed a 7.6 × 6.8 × 5.1–cm right upper pole kidney mass as shown in the Figure (left). Large subcapsular fluid collection was seen displacing the kidney anteriorly measuring 7.6 × 5.6 × 9.1 cm, signifying subcapsular hematoma. A significant amount of surrounding fatty stranding was present, suggesting a perirenal hemorrhage. The patient was subsequently admitted and stayed for a week to monitor ongoing bleeding with trends of hemoglobin and further evaluation. Because he was stable during his hospital stay, he was counseled to follow up with outpatient urology to monitor his kidney mass.

The patient’s pain progressed significantly, prompting him to visit the emergency department a week later, before his scheduled appointment at a urologist’s office. At this visit, his hemoglobin level dropped to 10.6 g/dL with stable kidney function, while urinalysis revealed hematuria. Abdomen pelvis CT with IV contrast at the emergency department showed an interval enlargement of a large right subscapular collection measuring 20 cm (previously 11 cm), and the cystic mass of the upper pole of the right kidney was now measuring 10.2 cm (previously 4.6 cm). There was also a new mass effect on the right hepatic lobe. Further, magnetic resonance imaging (MRI) of the abdomen with contrast revealed a right kidney posterior subcapsular hematoma measuring 18 × 13 × 11 cm with an exophytic right kidney upper pole mass measuring 9 × 10 × 7.8 cm within the hematoma superiorly as shown in the Figure (right). This feature was suggestive of renal carcinoma.
During the hospital stay, the patient’s blood pressure dropped below the normal range and he was volume resuscitated. His hemoglobin level dropped to 7.1 g/dL so he was transfused 1 unit of packed red blood cells. His platelet counts reached a maximum of 1216x103/μL, while his white blood cell count reached 25.19/μL, despite multiple negative cultures. CT-guided kidney biopsy was obtained and 800 cc of old blood was drained percut6aneously. While the old blood was negative for malignant cells, biopsy results revealed a poorly differentiated, malignant neoplasm. The patient also developed right pleural effusion and subsequently underwent a diagnostic thoracentesis. Analysis of the fluid revealed atypical malignant cells with similar immunohistochemical markers to that seen in the biopsy of the kidney mass. The patient underwent a right open radical nephroureterectomy. Postoperatively, the patient remained stable, and his biopsy reports showed undifferentiated renal carcinoma. Following the removal of the kidney mass, his platelet counts initially came down to normal range but subsequently rose again, possibly due to advanced malignancy and malignant pleural effusion.
Clinical Discussion
In 1856, Carl Wunderlich named a previously reported nontraumatic perirenal hematoma case as “spontaneous renal capsule apoplexy.” This eventually came to be called Wunderlich disease, formally referring to any spontaneous perirenal hematoma unrelated to trauma.4–6 The etiology of Wunderlich syndrome is mostly renal malignancies, with renal angiomyolipoma being the most common benign cause, while renal cell carcinoma is the most common malignant cause.3 Other malignant causes can include metastases, urothelial carcinoma, or renal sarcomas. Renal vascular diseases, such as polyarteritis nodosa, renal vein thrombosis, or renal artery aneurysms, are vascular causes, while there are also renal infections or renal cystic disorders that could lead to Wunderlich syndrome.4,7 There are also reported cases following the use of anticoagulants8 or end-stage kidney disease following uremic platelet dysfunction9 or acute pancreatitis.10 In the current case, the patient developed Wunderlich syndrome secondary to undifferentiated renal carcinoma.
Clinical manifestations vary depending on the amount of bleeding. The classic triad of flank pain, mass in the abdomen, and hypovolemic shock is present in only 20% of cases. Acutely developing flank pain is the most consistent symptom of this syndrome, present in about 67% of cases, followed by hematuria in around 40%, and hemorrhagic shock in around 26.5%.11,12 In this case, the patient had initially presented with flank pain. On subsequent hospitalization, he developed hematuria, hypovolemic shock, and a drop in hemoglobin level requiring IV fluids as well as a blood transfusion.
CT scan of the abdomen is the preferred initial imaging modality, with 100% sensitivity, because it can be used to see the cause of bleeding, simultaneously ruling out other causes.13,14 However, other cross-sectional imaging tools, such as ultrasonography and MRI, can also be considered.4 MRI can be considered when the initial CT imaging does not identify the source of bleeding, while ultrasonography is a highly sensitive modality to detect perinephric hematoma.3 In this case, the initial CT scan showed a mass but no signs of active bleeding. Thus, the patient was advised to have an outpatient follow-up with a urologist. However, due to his symptoms, he could not wait until his appointment and was subsequently readmitted and evaluated.
Thrombocytosis has been associated with renal malignancies and platelet counts are sometimes used for prognostic assessment. The platelet count can be correlated with the aggressive nature of the tumor and a raised count could indicate advanced carcinomas and poor prognosis.15,16 In the current case, the platelet trends showed gradually rising platelet counts, reaching a maximum of 1216 x103 /μL. However, following tumor removal, the platelet count dropped to baseline. His platelet counts started to rise as he had malignant pleural effusion, indicating metastasis and advanced malignancy.
Treatment of Wunderlich syndrome depends on the underlying cause and the condition of the patient. A laparoscopic approach can lead to the seeding of tumors in the port site in cases of kidney malignancies; hence, open surgery is the preferred option. For stable patients, conservative therapy, partial or complete nephrectomy, or minimally invasive procedures such as angiographic embolization to control the bleeding can be performed.2,14 In this case, the patient underwent a right open radical nephroureterectomy due to expanding hematoma and concerns for malignancy. The patient will be evaluated by oncology for possible chemotherapy and radiotherapy.
Conclusion
The current case presented with flank pain and was later found to have Wunderlich syndrome, secondary to renal malignancy. Acutely developing flank pain is more common with Wunderlich syndrome than a typical triad of flank pain, flank mass, or hypovolemic shock. Consideration of this syndrome can be easily overlooked because of its rarity, and it can be life-threatening if not promptly and aggressively treated. Thus, watching for triads to diagnose can sometimes be dangerous. Once a diagnosis is made, it is crucial to find the etiology because sinister causes, such as kidney malignancies, need to be ruled out. If Wunderlich syndrome is found to be present, it is essential to rapidly intervene, as well as inform the patient about the very serious nature and potentially fatal consequences of delaying any treatment.
Funding sources
None.
Conflict of interest
None reported.